

Botulinum Toxin A: A Novel Therapeutic Modality for Upper Extremity Chronic Regional Pain Syndrome
- PMID: 30534480
- PMCID: PMC6250468
- DOI: 10.1097/GOX.0000000000001847
Botulinum Toxin A: A Novel Therapeutic Modality for Upper Extremity Chronic Regional Pain Syndrome
Abstract
Background: Complex regional pain syndromes (CRPS) is a disease that is poorly understood. It is a chronic pain syndrome characterized by sympathetic disruptions as well as CNS sensitization. Botulinum Toxin-A has been shown to have efficacy in Raynaud's as well as other neuropathic pain disorders. Perhaps BTX-A warrants experimentation in the treatment of CRPS.
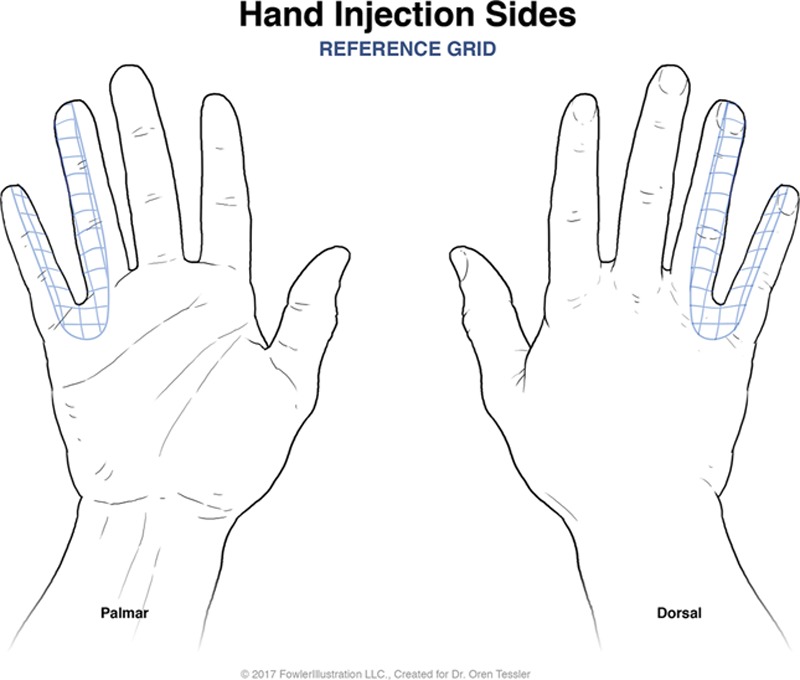
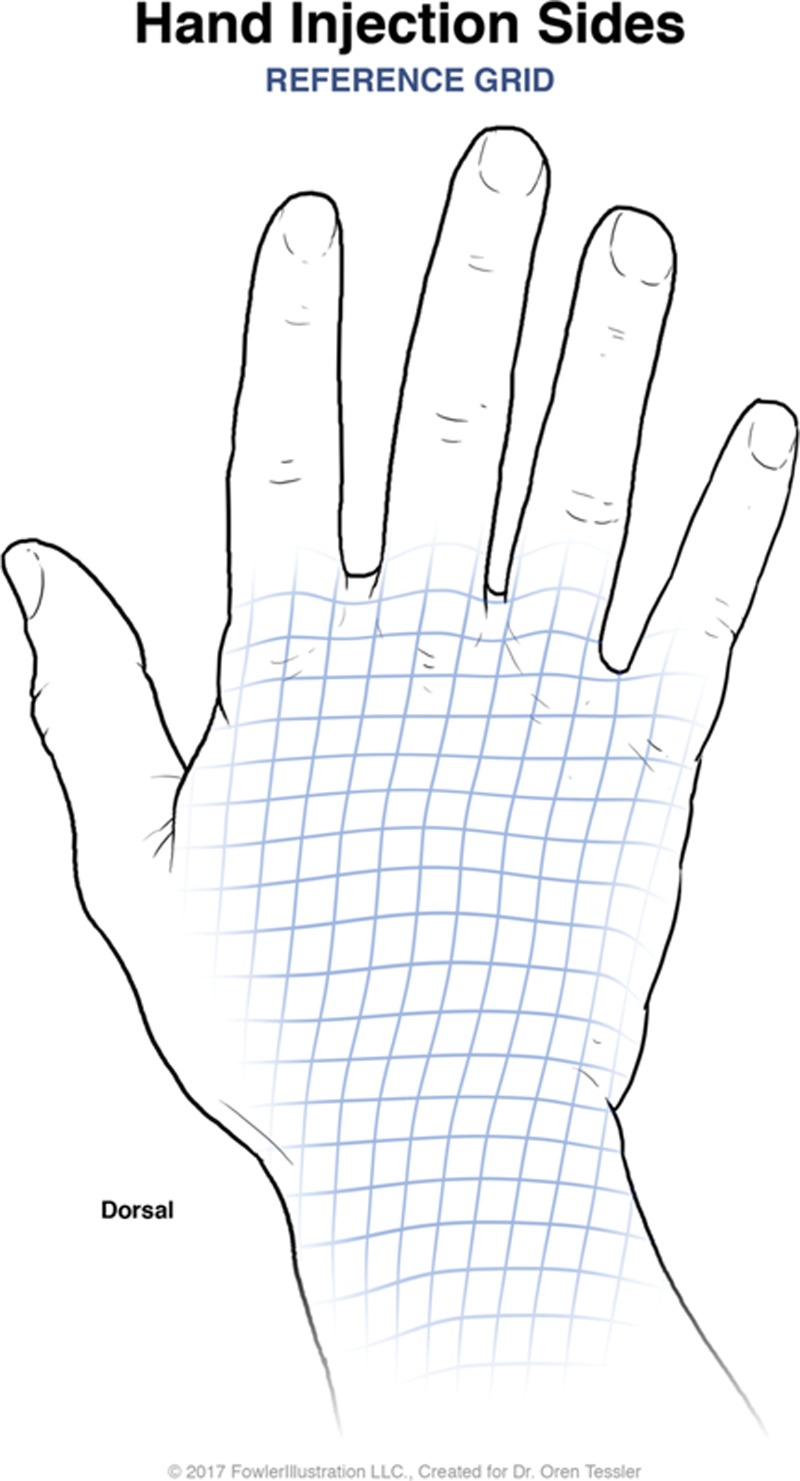
Methods: Patients with CRPS refractory to 2 or more regional sympathetic nerve blocks in 2007 were included in the study. Patient's were asked to rank their initial pain on a visual analog scale of 0 to 10 (10 being the worst pain). "Tenderness maps" were marked on patient's areas of most pain in 1 by 1 centimeter grids. Each box on the grid was injected with 10 IU of BTX-A after nerve blocks with 1% lidocaine. Treatment sessions occured on a monthly basis with VAS pain scores being re-assessed immediately before the new treatment. t Test, linear regression, and Cohen's D-test were used to analyze the correlation of the data.
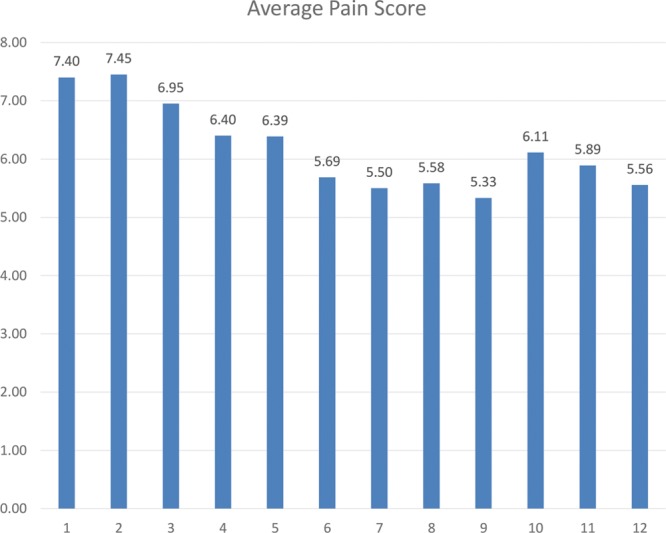
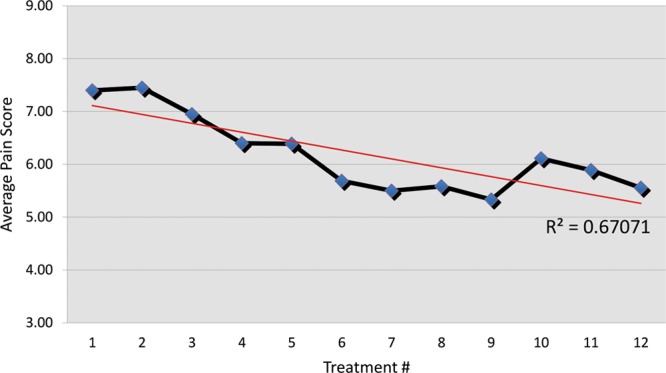
Results: Study sample was 20 patients. Etiology of CRPS was 6 amputations, 4 crush injuries, 4 penetrating injuries, and 2 lacerations. Average pain reduction on VAS scale achieved was 2.05 points. Average percentage pain reduction was 22.94%. Cohen's D Test also showed a meaningful difference with a score of 1.01. Linear regression R2 = 0.491. Maximum pain reduction, on average, was achieved by treatment 9.
Conclusion: Despite the esoteric etiology of CRPS, BTX-A has a well-demonstrated mechanism of effect. BTX-A should be further explored as a treatment modality for CRPS.
Figures
References
-
- O’Connel N, Wand B, McAuley J, et al. Interventions for treating pain and disability in adults with complex regional pain syndrome- an overview of systematic reviews (Review). Cochrane Database Syst Rev. 2013;4:1. doi: 10.1002/14651858.CD009416. pub2. www.cochranelibrary.com. - PMC - PubMed
-
- Borchers AT, Gershwin ME. Complex regional pain syndrome: a comprehensive and critical review. Autoimmun Rev. 2014;13:242. - PubMed
-
- Galer BS, Jensen M. Neglect-like symptoms in complex regional pain syndrome: results of a self-administered survey. J Pain Symptom Manage. 1999;18:213. - PubMed
-
- de Mos M, de Bruijn AG, Huygen FJ, et al. The incidence of complex regional pain syndrome: a population-based study. Pain. 2007;129:12. - PubMed
-
- Neumeister MW. Botulinum toxin type A in the treatment of Raynaud’s phenomenon. J Hand Surg Am. 2010;35:2085. - PubMed
LinkOut - more resources
Full Text Sources