

Surgical Algorithm for Neuroma Management: A Changing Treatment Paradigm
- PMID: 30534497
- PMCID: PMC6250458
- DOI: 10.1097/GOX.0000000000001952
Surgical Algorithm for Neuroma Management: A Changing Treatment Paradigm
Abstract
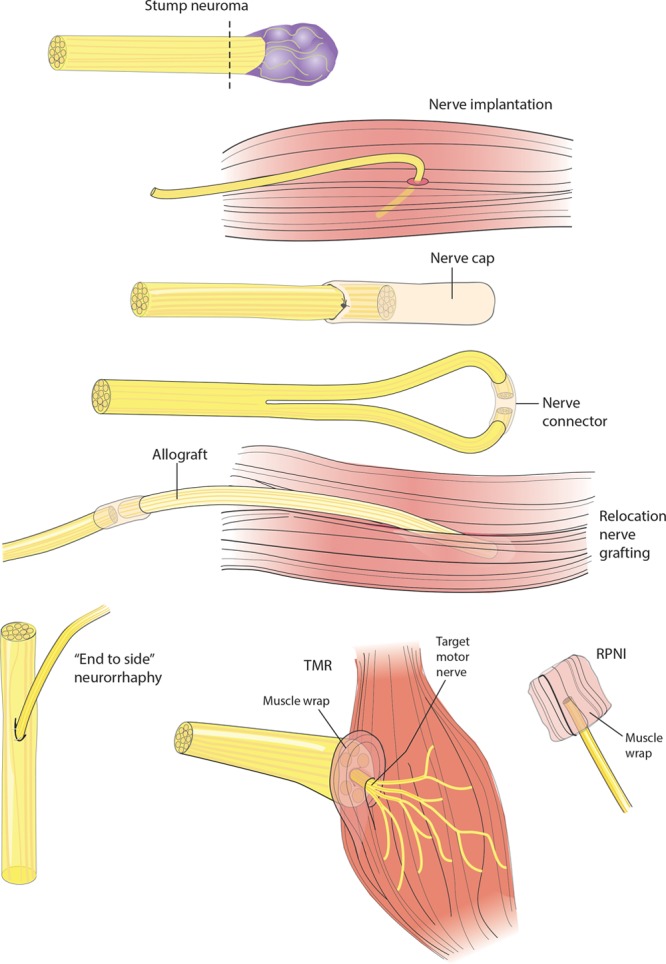
Successful treatment of the painful neuroma is a particular challenge to the nerve surgeon. Historically, symptomatic neuromas have primarily been treated with excision and implantation techniques, which are inherently passive and do not address the terminal end of the nerve. Over the past decade, the surgical management of neuromas has undergone a paradigm shift synchronous with the development of contemporary techniques aiming to satisfy the nerve end. In this article, we describe the important features of surgical treatment, including the approach to diagnosis with consideration of neuroma type and the decision of partial versus complete neuroma excision. A comprehensive list of the available surgical techniques for management following neuroma excision is presented, the choice of which is often predicated upon the availability of the terminal nerve end for reconstruction. Techniques for neuroma reconstruction in the presence of an intact terminal nerve end include hollow tube reconstruction and auto- or allograft nerve reconstruction. Techniques for neuroma management in the absence of an intact or identifiable terminal nerve end include submuscular or interosseous implantation, centro-central neurorrhaphy, relocation nerve grafting, nerve cap placement, use of regenerative peripheral nerve interface, "end-to-side" neurorrhaphy, and targeted muscle reinnervation. These techniques can be further categorized into passive/ablative and active/reconstructive modalities. The nerve surgeon must be aware of available treatment options and should carefully choose the most appropriate intervention for each patient. Comparative studies are lacking and will be necessary in the future to determine the relative effectiveness of each technique.
Figures



References
-
- Stokvis A, van der Avoort DJ, van Neck JW, et al. Surgical management of neuroma pain: a prospective follow-up study. Pain. 2010;151:862. - PubMed
-
- Lee SK, Wolfe SW. Peripheral nerve injury and repair. J Am Acad Orthop Surg. 2000;8:243. - PubMed
-
- Fried K, Govrin-Lippmann R, Rosenthal F, et al. Ultrastructure of afferent axon endings in a neuroma. J Neurocytol. 1991;20:682. - PubMed
-
- Vlot MA, Wilkens SC, Chen NC, et al. Symptomatic neuroma following initial amputation for traumatic digital amputation. J Hand Surg Am. 2018;43:86.e1. - PubMed
-
- Geraghty TJ, Jones LE. Painful neuromata following upper limb amputation. Prosthet Orthot Int. 1996;20:176. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous