

Clinical presentation and survival of childhood hypertrophic cardiomyopathy: a retrospective study in United Kingdom
- PMID: 30535072
- PMCID: PMC6427088
- DOI: 10.1093/eurheartj/ehy798
Clinical presentation and survival of childhood hypertrophic cardiomyopathy: a retrospective study in United Kingdom
Abstract
Aims: Understanding the spectrum of disease, symptom burden and natural history are essential for the management of children with hypertrophic cardiomyopathy (HCM). The effect of changing screening practices over time has not previously been studied. This study describes the clinical characteristics and outcomes of childhood HCM over four decades in a well-characterized United Kingdom cohort.
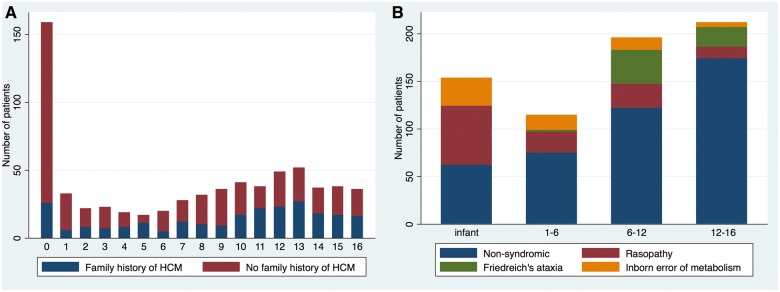
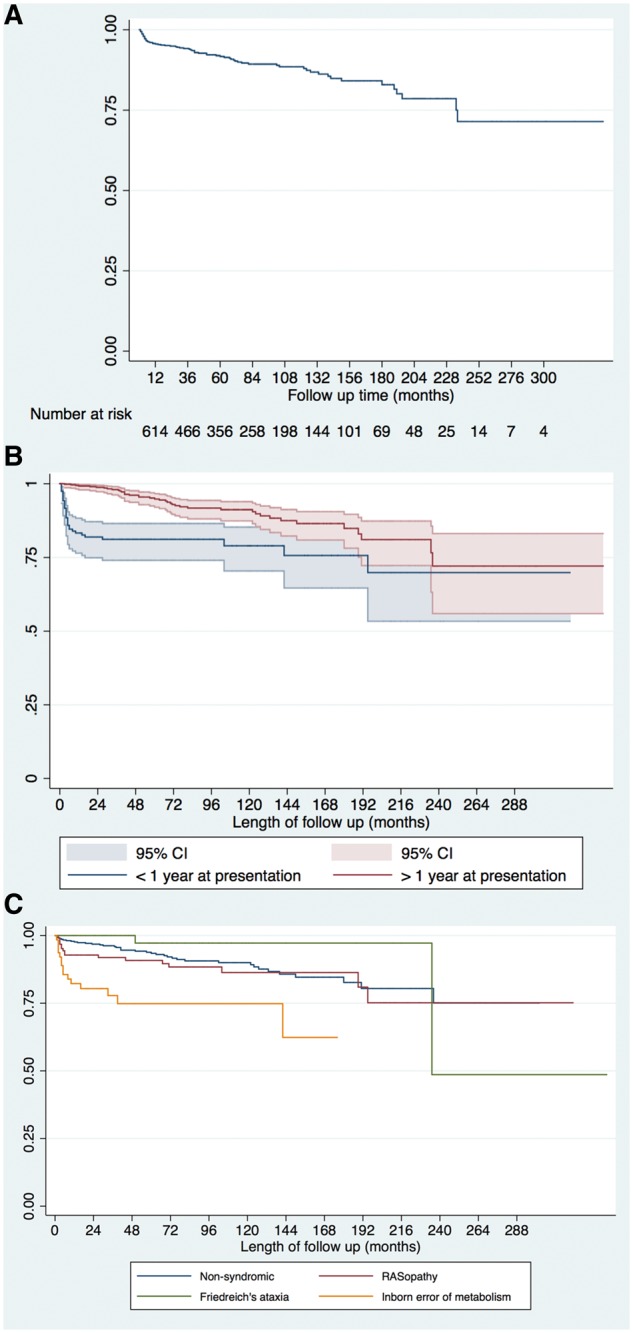
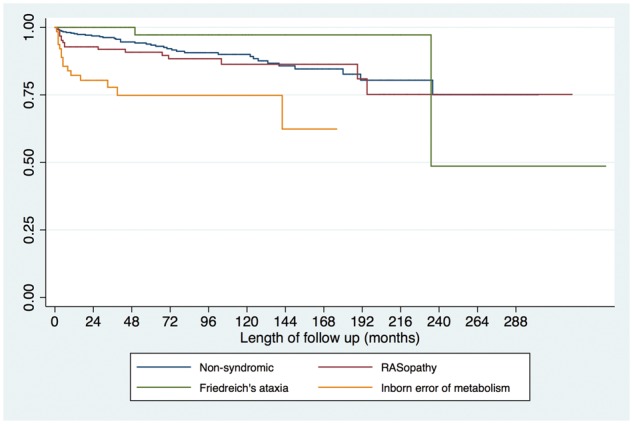
Methods and results: Six hundred and eighty-seven patients with HCM presented at a median age of 5.2 years (range 0-16). Aetiology was: non-syndromic (n = 433, 63%), RASopathy (n = 126, 18.3%), Friedreich's ataxia (n = 59, 8.6%) or inborn errors of metabolism (IEM) (n = 64, 9%). In infants (n = 159, 23%) underlying aetiology was more commonly a RASopathy (42% vs. 11.2%, P < 0.0001) or IEM (18.9% vs. 6.4% P < 0.0001). In those with familial disease, median age of presentation was higher (11 years vs. 6 years, P < 0.0001), 141 (58%) presented <12 years. Freedom from death or transplantation was 90.6% (87.9-92.7%) at 5 years (1.5 per 100 patient years) with no era effect. Mortality was most frequently sudden cardiac death (SCD) (n = 20, 2.9%). Children diagnosed during infancy or with an IEM had a worse prognosis (5-year survival 80.5% or 66.4%). Arrhythmic events occurred at a rate of 1.2 per 100 patient years and were more likely in non-syndromic patients (n = 51, 88%).
Conclusion: This national study describes a heterogeneous disease whose outcomes depend on the age of presentation and aetiology. Overall mortality and SCD rates have not changed over time, but they remain higher than in adults with HCM, with events occurring in syndromic and non-syndromic patients.
Keywords: Aetiology; Hypertrophic cardiomyopathy; Survival; United Kingdom.
© The Author(s) 2018. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
The hypertrophic cardiomyopathy paradox: better with age.Eur Heart J. 2019 Mar 21;40(12):994-996. doi: 10.1093/eurheartj/ehy889. Eur Heart J. 2019. PMID: 30629161 No abstract available.
References
-
- Arola A, Jokinen E, Ruuskanen O, Saraste M, Pesonen E, Kuusela AL, Tikanoja T, Paavilainen T, Simell O.. Epidemiology of idiopathic cardiomyopathies in children and adolescents. A nationwide study in Finland. Am J Epidemiol 1997;146:385–393. - PubMed
-
- Lipshultz SE, Sleeper LA, Towbin JA, Lowe AM, Orav EJ, Cox GF, Lurie PR, McCoy KL, McDonald MA, Messere JE, Colan SD.. The incidence of paediatric cardiomyopathy in two regions of the United States. N Engl J Med 2003;348:1647–1655. - PubMed
-
- Nugent AW, Daubeney PE, Chondros P, Carlin JB, Cheung M, Wilkinson LC, Davis AM, Kahler SG, Chow CW, Wilkinson JL, Weintraub RG.. The epidemiology of childhood cardiomyopathy in Australia. N Engl J Med 2003;348:1639–1646. - PubMed
-
- Kaski JP, Syrris P, Esteban MT, Jenkins S, Pantazis A, Deanfield JE, McKenna WJ, Elliott PM.. Prevalence of sarcomere protein gene mutations in preadolescent children with hypertrophic cardiomyopathy. Circ Cardiovasc Genet 2009;2:436–441. - PubMed
-
- Colan SD, Lipshultz SE, Lowe AM, Sleeper LA, Messere J, Cox GF, Lurie PR, Orav EJ, Towbin JA.. Epidemiology and cause-specific outcome of hypertrophic cardiomyopathy in children: findings from the Paediatric Cardiomyopathy Registry. Circulation 2007;115:773–781. - PubMed
