

Effect of Oral Alfacalcidol on Clinical Outcomes in Patients Without Secondary Hyperparathyroidism Receiving Maintenance Hemodialysis: The J-DAVID Randomized Clinical Trial
- PMID: 30535217
- PMCID: PMC6583075
- DOI: 10.1001/jama.2018.17749
Effect of Oral Alfacalcidol on Clinical Outcomes in Patients Without Secondary Hyperparathyroidism Receiving Maintenance Hemodialysis: The J-DAVID Randomized Clinical Trial
Abstract
Importance: Patients with chronic kidney disease have impaired vitamin D activation and elevated cardiovascular risk. Observational studies in patients treated with hemodialysis showed that the use of active vitamin D sterols was associated with lower risk of all-cause mortality, regardless of parathyroid hormone levels.
Objective: To determine whether vitamin D receptor activators reduce cardiovascular events and mortality in patients without secondary hyperparathyroidism undergoing hemodialysis.
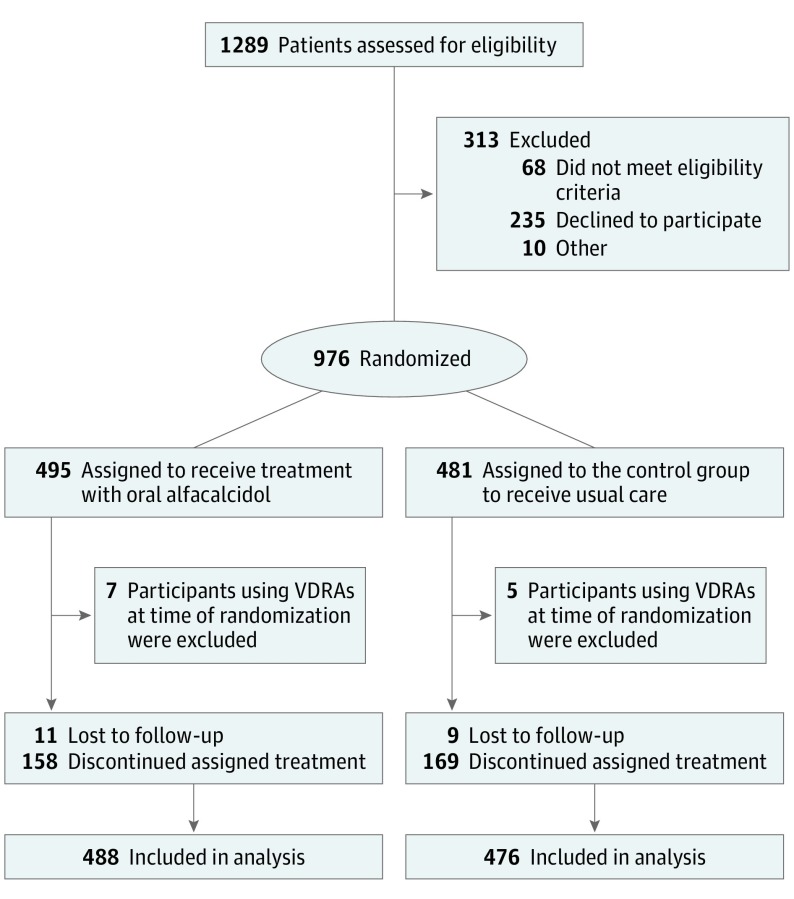
Design, setting, and participants: Randomized, open-label, blinded end point multicenter study of 1289 patients in 207 dialysis centers in Japan. The study included 976 patients receiving maintenance hemodialysis with serum intact parathyroid hormone levels less than or equal to 180 pg/mL. The first and last participants were enrolled on August 18, 2008, and January 26, 2011, respectively. The final date of follow-up was April 4, 2015.
Interventions: Treatment with 0.5 μg of oral alfacalcidol per day (intervention group; n = 495) vs treatment without vitamin D receptor activators (control group; n = 481).
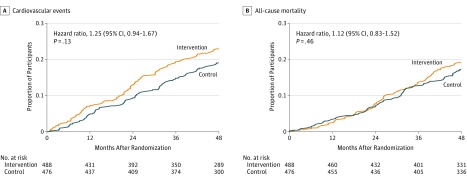
Main outcomes and measures: The primary outcome was a composite measure of fatal and nonfatal cardiovascular events, including myocardial infarctions, hospitalizations for congestive heart failure, stroke, aortic dissection/rupture, amputation of lower limb due to ischemia, and cardiac sudden death; coronary revascularization; and leg artery revascularization during 48 months of follow-up. The secondary outcome was all-cause death.
Results: Among 976 patients who were randomized from 108 dialysis centers, 964 patients were included in the intention-to-treat analysis (median age, 65 years; 386 women [40.0%]), and 944 (97.9%) completed the trial. During follow-up (median, 4.0 years), the primary composite outcome of cardiovascular events occurred in 103 of 488 patients (21.1%) in the intervention group and 85 of 476 patients (17.9%) in the control group (absolute difference, 3.25% [95% CI, -1.75% to 8.24%]; hazard ratio, 1.25 [95% CI, 0.94-1.67]; P = .13). There was no significant difference in the secondary outcome of all-cause mortality between the groups (18.2% vs 16.8%, respectively; hazard ratio, 1.12 [95% CI, 0.83-1.52]; P = .46). Of the 488 participants in the intervention group, 199 (40.8%) experienced serious adverse events that were classified as cardiovascular, 64 (13.1%) experienced adverse events classified as infection, and 22 (4.5%) experienced malignancy-related serious adverse events. Of 476 participants in the control group, 191 (40.1%) experienced cardiovascular-related serious adverse events, 63 (13.2%) experienced infection-related serious adverse events, and 21 (4.4%) experienced malignancy-related adverse events.
Conclusions and relevance: Among patients without secondary hyperparathyroidism undergoing maintenance hemodialysis, oral alfacalcidol compared with usual care did not reduce the risk of a composite measure of select cardiovascular events. These findings do not support the use of vitamin D receptor activators for patients such as these.
Trial registration: UMIN-CTR Identifier: UMIN000001194.
Conflict of interest statement
Figures
Comment in
-
Vitamin D Receptor Agonists for Patients Undergoing Hemodialysis.JAMA. 2018 Dec 11;320(22):2319-2321. doi: 10.1001/jama.2018.17477. JAMA. 2018. PMID: 30535205 No abstract available.
-
Does alfacalcidol reduce cardiovascular complications in hemodialysis patients?Ann Transl Med. 2019 Apr;7(8):167. doi: 10.21037/atm.2019.03.26. Ann Transl Med. 2019. PMID: 31168448 Free PMC article. No abstract available.
References
-
- Sarnak MJ, Levey AS, Schoolwerth AC, et al. . Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension. 2003;42(5):1050-1065. doi:10.1161/01.HYP.0000102971.85504.7c - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
