

Prospective, randomized, controlled, open-label study to compare efficacy of a mineral-rich solution vs normal saline after complete ethmoidectomy
- PMID: 30536161
- PMCID: PMC6394433
- DOI: 10.1007/s00405-018-5232-9
Prospective, randomized, controlled, open-label study to compare efficacy of a mineral-rich solution vs normal saline after complete ethmoidectomy
Abstract
Purposes: The purpose of this study was to compare the efficacy of a mineral-rich solution vs normal saline solution (0.9% NaCl) following endoscopic complete bilateral ethmoidectomy.
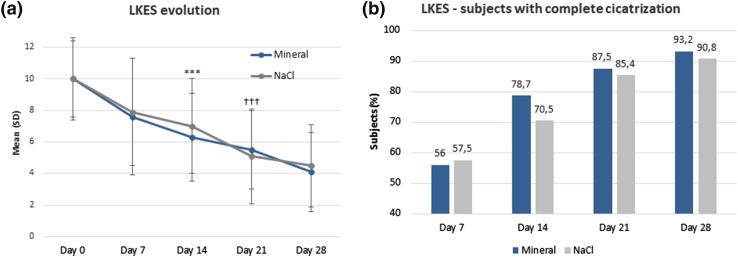
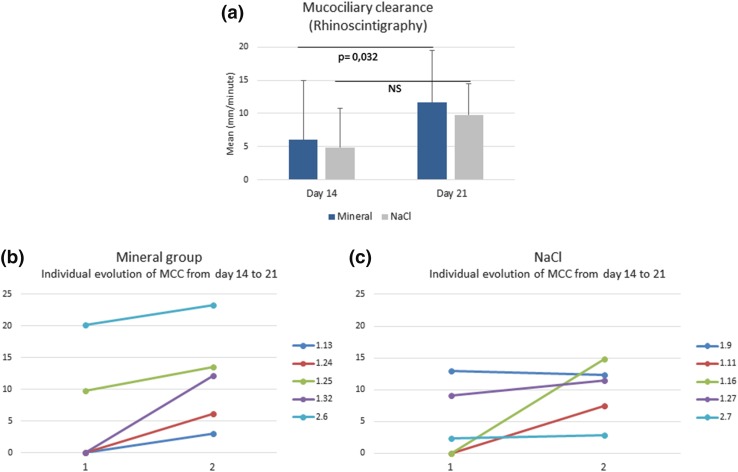
Methods: This was a prospective, multicenter, randomized, controlled, open-label trial in subjects suffering from steroid-resistant sinonasal polyposis. Adults performed 4 nasal irrigations of mineral or saline solutions daily for 28 days. Evaluations included subject-reported RHINO quality of life (QoL) and NOSE scores, tolerability, and satisfaction, the Lund-Kennedy endoscopic score and assessments of crusting, secretions and mucociliary clearance (rhinoscintigraphy).
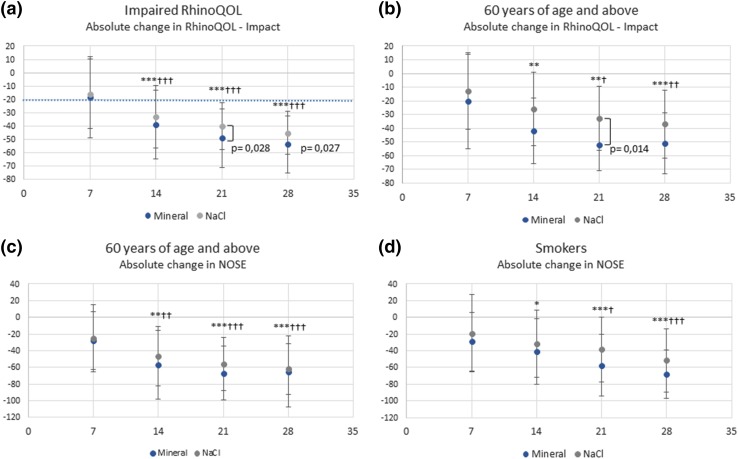
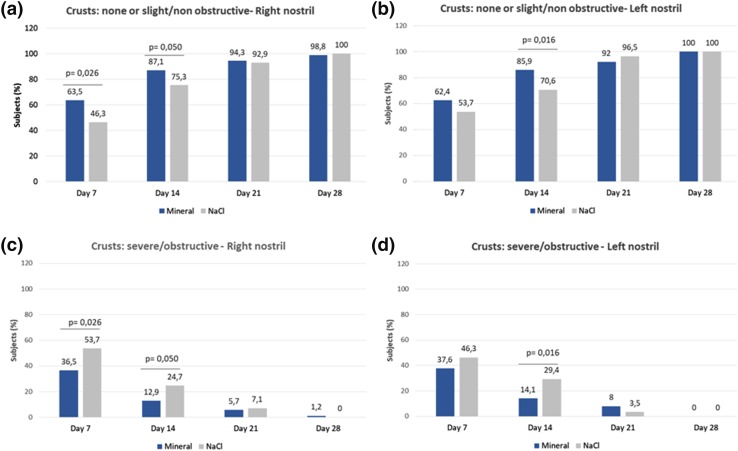
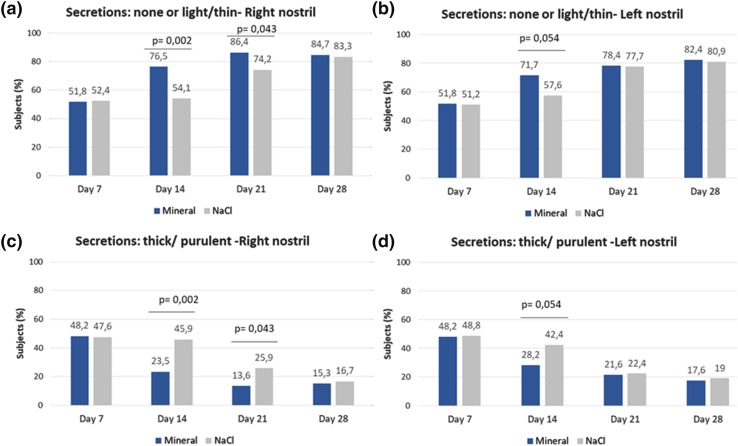
Results: A total of 189 subjects were randomized. Clinically relevant improvements (> 20 points) in RhinoQOL and NOSE scores were measured in both groups without any significant inter-group difference. Among the subjects with impaired RhinoQOL at pre-inclusion, the change in Impact-RhinoQOL score was significantly superior in mineral-rich vs saline solution at day 21 (p = 0.028) and day 28 (p = 0.027). The Lund-Kennedy score continuously improved in both groups earlier with the mineral-rich solution. Crusts were significantly fewer in number and less severe/obstructive in patients receiving mineral-rich vs saline solution at day 7 (p = 0.026) and day 14 (p = 0.016). Furthermore, secretions disappeared significantly more quickly and were less thick/purulent with mineral-rich solution at day 14 (p = 0.002) and day 21 (p = 0.043). Less epistaxis was reported in the mineral vs saline solution (p = 0.008 at day 21).
Conclusions: Our findings indicate that the composition of a nasal irrigation solution influences endoscopic scores and QoL after sinus surgery for patients over 60, those with an initially poor QoL and higher symptom score, and smokers.
Keywords: Chronic rhinosinusitis; Lund–Kennedy endoscopic score; Mucociliary clearance; Nasal irrigation; Nasal polyposis.
Figures
Similar articles
-
Efficacy of buffered hypertonic seawater in different phenotypes of chronic rhinosinusitis with nasal polyps after endoscopic sinus surgery: a randomized double-blind study.Am J Otolaryngol. 2020 Sep-Oct;41(5):102554. doi: 10.1016/j.amjoto.2020.102554. Epub 2020 May 26. Am J Otolaryngol. 2020. PMID: 32521299 Clinical Trial.
-
Comparison of effects of baby shampoo vs. saline irrigation on endoscopic sinus surgery outcomes and quality of life.Auris Nasus Larynx. 2021 Jun;48(3):408-414. doi: 10.1016/j.anl.2020.08.009. Epub 2020 Aug 26. Auris Nasus Larynx. 2021. PMID: 32859445
-
Effect of Budesonide Added to Large-Volume, Low-pressure Saline Sinus Irrigation for Chronic Rhinosinusitis: A Randomized Clinical Trial.JAMA Otolaryngol Head Neck Surg. 2018 Jul 1;144(7):605-612. doi: 10.1001/jamaoto.2018.0667. JAMA Otolaryngol Head Neck Surg. 2018. PMID: 29879268 Free PMC article. Clinical Trial.
-
Saline nasal irrigations for chronic rhinosinusitis: From everyday practice to evidence-based medicine. An update.Int J Immunopathol Pharmacol. 2018 Jan-Dec;32:2058738418802676. doi: 10.1177/2058738418802676. Int J Immunopathol Pharmacol. 2018. PMID: 30350744 Free PMC article. Review.
-
Benefits of nasal saline treatment in acute rhinosinusitis: Systematic review and meta-analysis.Int Forum Allergy Rhinol. 2022 Aug;12(8):1006-1017. doi: 10.1002/alr.22957. Epub 2022 Jan 14. Int Forum Allergy Rhinol. 2022. PMID: 34971301
Cited by
-
Seawater nasal wash to reduce symptom duration and viral load in COVID-19 and upper respiratory tract infections: a randomized controlled multicenter trial.Eur Arch Otorhinolaryngol. 2024 Jul;281(7):3625-3637. doi: 10.1007/s00405-024-08518-y. Epub 2024 Feb 20. Eur Arch Otorhinolaryngol. 2024. PMID: 38376591 Free PMC article. Clinical Trial.
-
Safety and Impact of Nasal Lavages During Viral Infections Such as SARS-CoV-2.Ear Nose Throat J. 2021 Apr;100(2_suppl):188S-191S. doi: 10.1177/0145561320950491. Epub 2020 Aug 27. Ear Nose Throat J. 2021. PMID: 32853040 Free PMC article. Review. No abstract available.
References
-
- Desrosiers M, Evans GA, Keith PK, et al. Canadian clinical practice guidelines for acute and chronic rhinosinusitis. J Otolaryngol Head Neck Surg. 2011;40(Suppl 2):S99–S193. - PubMed
-
- Fokkens WJ, Lund VJ, Mullol J, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2012. Rhinol Suppl. 2012;23:3. - PubMed
-
- SFORL (2001) Les thérapeutiques peropératoires en chirurgie endonasale. Cachan: LOb Conseil. https://www.orlfrance.org/wp-content/uploads/2017/06/RPC1_chir_endonasal.... Accessed Feb 2018
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
