

Long-term macrolide treatment for the prevention of acute exacerbations in COPD: a systematic review and meta-analysis
- PMID: 30538443
- PMCID: PMC6254503
- DOI: 10.2147/COPD.S181246
Long-term macrolide treatment for the prevention of acute exacerbations in COPD: a systematic review and meta-analysis
Abstract
Background: Acute exacerbation of COPD (AECOPD) is associated with an increased hospitalization and mortality. Azithromycin and erythromycin are the recommended drugs to reduce the risk of exacerbations. However, the most suitable duration of therapy and drug-related adverse events are still a matter of debate. The aim of this meta-analysis was to assess the current evidence regarding the efficacy and safety of long-term macrolide treatment for COPD.
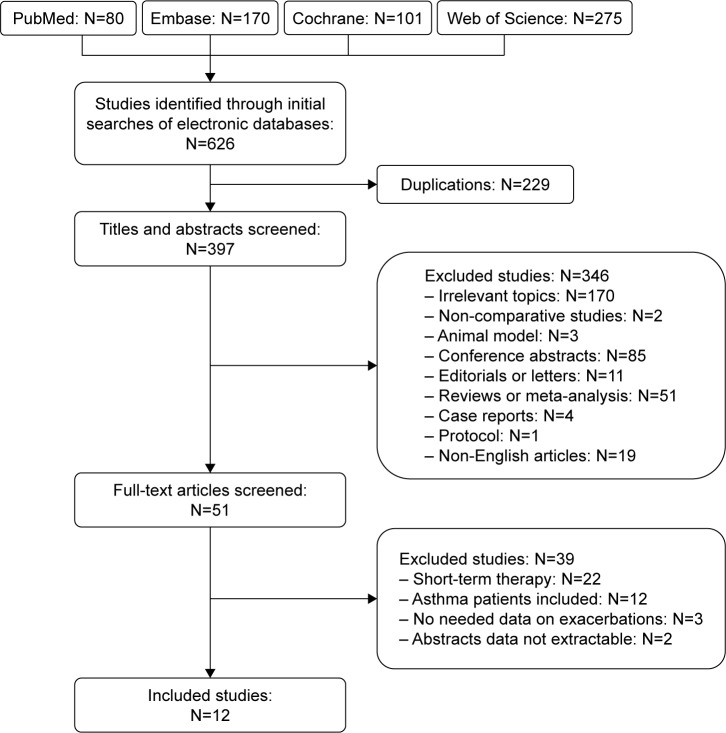
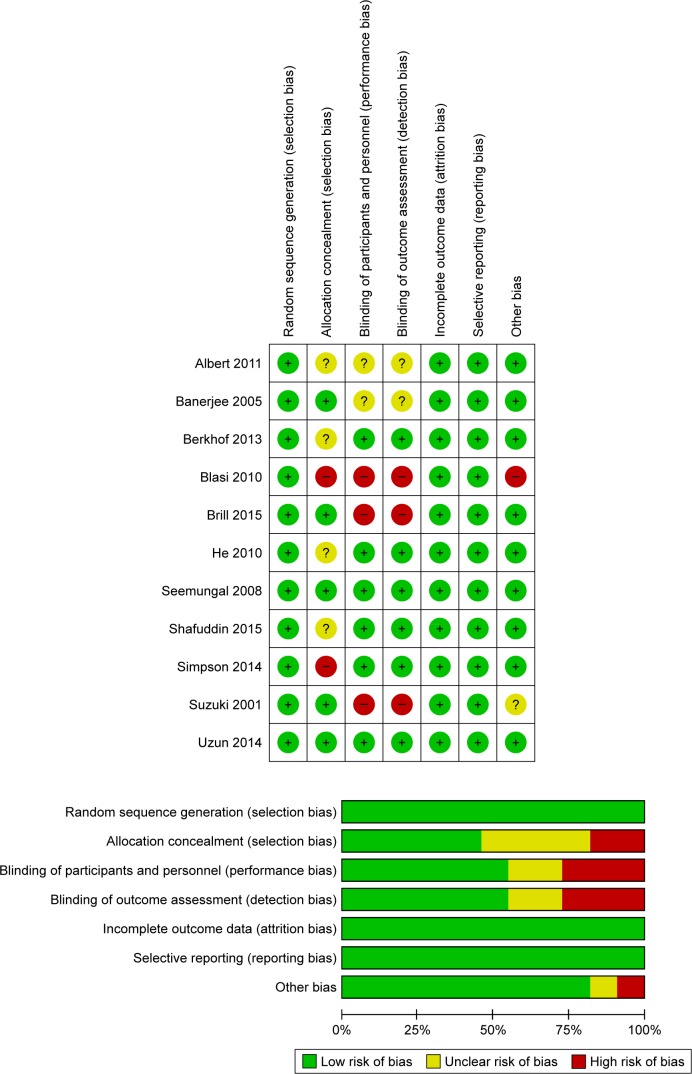
Materials and methods: We comprehensively searched PubMed, Embase, the Cochrane Library, and the Web of Science and performed a systematic review and cumulative meta-analysis of all randomized controlled trials (RCTs) and retrospective studies.
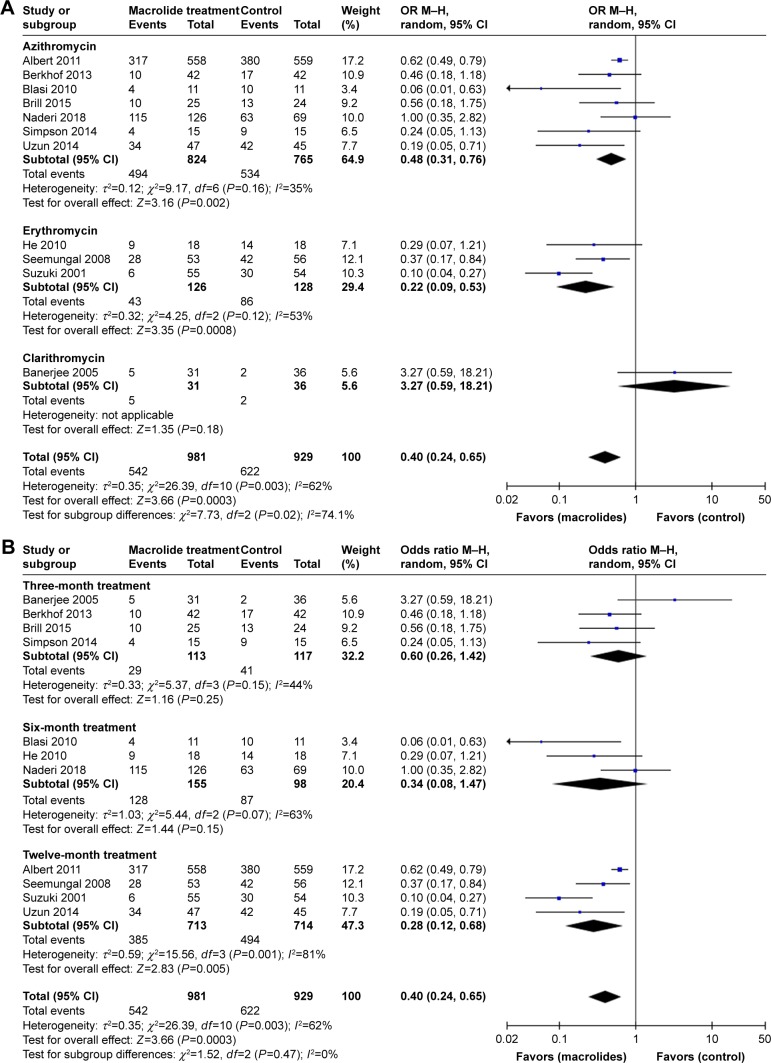
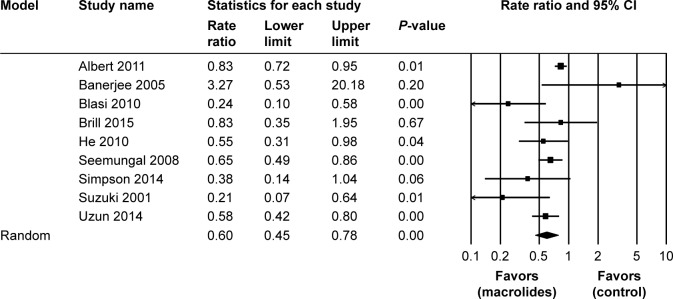
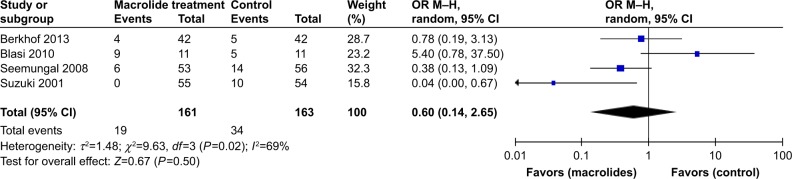
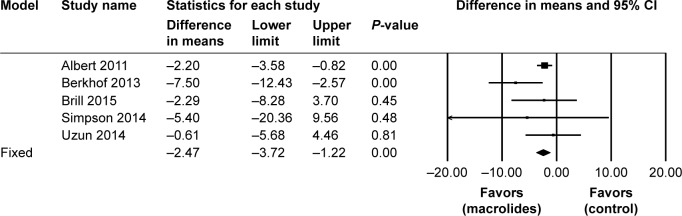
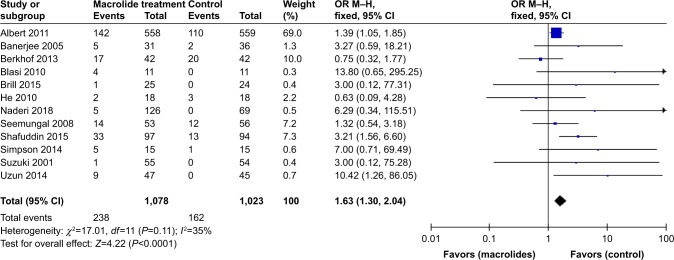
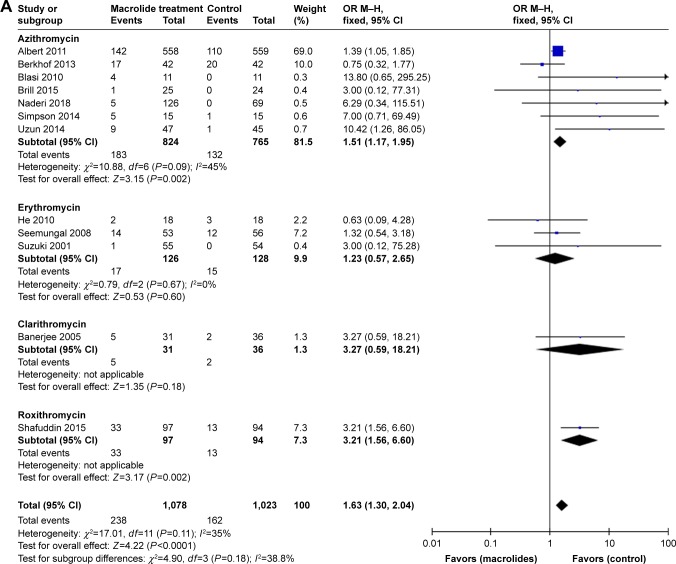
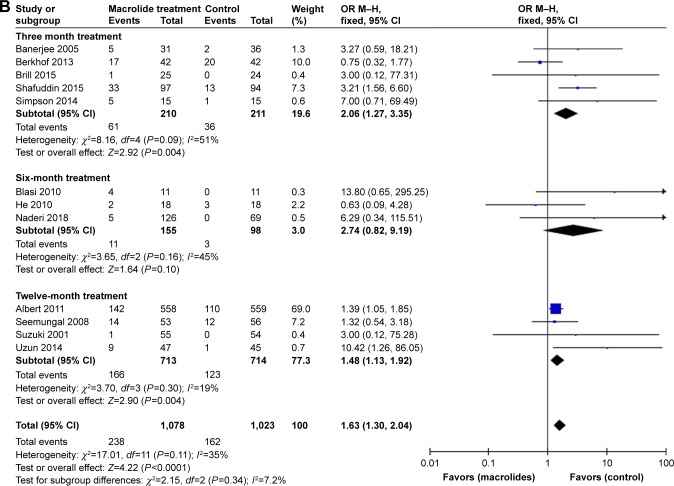
Results: Eleven RCTs and one retrospective study including a total of 2,151 cases were carried out. Long-term macrolide treatment significantly reduced the total number of cases with one or more exacerbations (OR=0.40; 95% CI=0.24-0.65; P<0.01) and the rate of exacerbations per patient per year (risk ratio [RR]=0.60; 95% CI=0.45-0.78; P<0.01). Subgroup analyses showed that the minimum duration for drug efficacy for both azithromycin and erythromycin therapy was 6 months. In addition, macrolide therapy could improve the St George Respiratory Questionnaire (SGRQ) total score (P<0.01) but did not achieve the level of clinical significance. The frequency of hospitalizations was not significantly different between the treatment and control groups (P=0.50). Moreover, chronic azithromycin treatment was more likely to increase adverse events (P<0.01).
Conclusion: Prophylactic azithromycin or erythromycin treatment has a significant effect in reducing the frequency of AECOPD in a time-dependent manner. However, long-term macrolide treatment could increase the occurrence of adverse events and macrolide resistance. Future large-scale, well-designed RCTs with extensive follow-up are required to identify patients in whom the benefits outweigh risks.
Keywords: AECOPD; adverse events; azithromycin; macrolide.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures

References
-
- GOLD Executive Committee [homepage on the Internet] Global strategy for the diagnosis management and prevention of chronic obstructive pulmonary disease. 2018. [Accessed October 25, 2018]. Available from: http://goldcopd.com.
-
- Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. - PubMed
-
- Vestbo J, Edwards LD, Scanlon PD, et al. Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med. 2011;365(13):1184–1192. - PubMed
-
- Barnes PJ. Inhaled corticosteroids in COPD: a controversy. Respiration. 2010;80(2):89–95. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
