

Mortality in people with dementia, delirium, and unspecified cognitive impairment in the general hospital: prospective cohort study of 6,724 patients with 2 years follow-up
- PMID: 30538578
- PMCID: PMC6257080
- DOI: 10.2147/CLEP.S174807
Mortality in people with dementia, delirium, and unspecified cognitive impairment in the general hospital: prospective cohort study of 6,724 patients with 2 years follow-up
Abstract
Purpose: Cognitive impairment is common in older people admitted to hospital, but the outcomes are generally poorly understood, and previous research has shown inconsistent associations with mortality depending on the type of cognitive impairment examined and duration of follow-up. This study examines mortality in older people with any cognitive impairment during acute hospital admission.
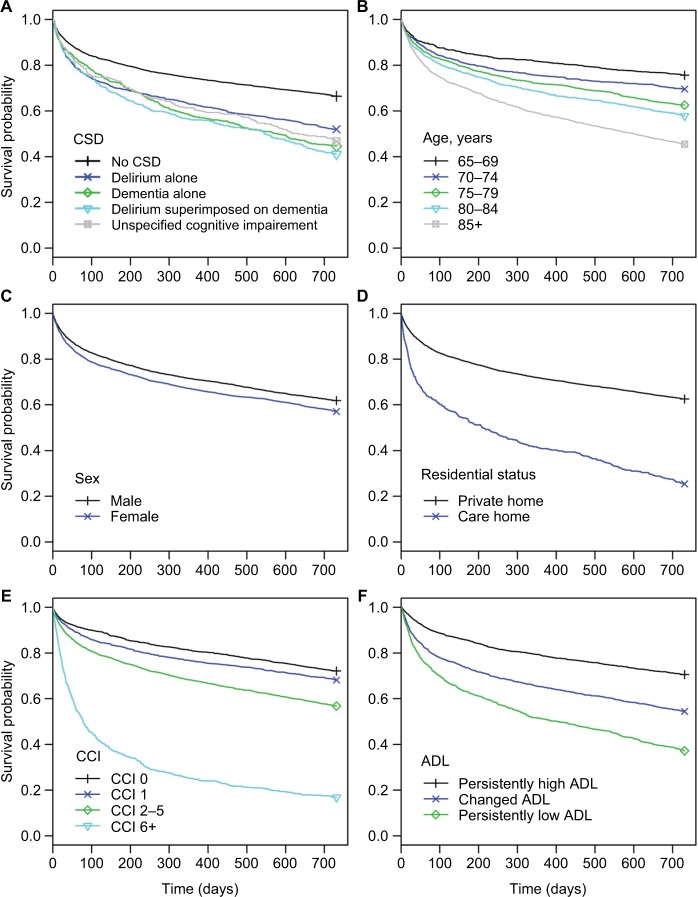
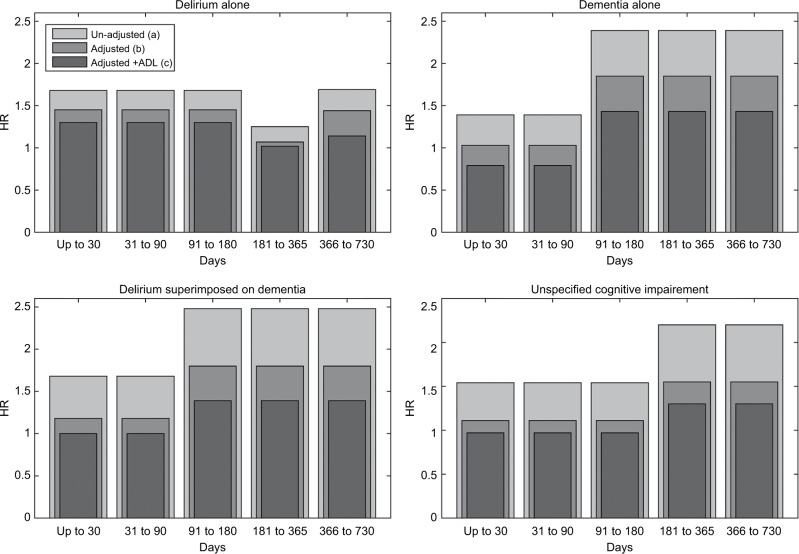
Patients and methods: Prospective cohort of 6,724 people aged ≥65 years with a structured cognitive assessment on acute admission were included in this study. Cognitive spectrum disorder (CSD) was defined as delirium alone, known dementia alone, delirium superimposed on known dementia, or unspecified cognitive impairment. Mortality associated with different types of CSD was examined using a non-proportional hazards model with 2-year follow-up.
Results: On admission, 35.4% of patients had CSD, of which 52.6% died within 2 years. After adjustment for demographics and comorbidity, delirium alone was associated with increased mortality in the 6 months post-admission (HR =1.45, 95% CI 1.28-1.65) and again after 1 year (HR =1.44, 95% CI 1.17-1.77). Patients with known dementia (alone or with superimposed delirium) had increased mortality only after 3 months from admission (HR =1.85, 95% CI 1.56-2.18 and HR =1.80, 95% CI 1.52-2.14) compared with patients with unspecified cognitive impairment after 6 months (HR =1.55, 95% CI 1.21-1.99). Similar but partially attenuated associations were seen after adjustment for functional ability.
Conclusion: Mortality post-admission is high in older people with CSD. Immediate risk is highest in those with delirium, while dementia or unspecified cognitive impairment is associated with medium- to long-term risk. These findings suggest that individuals without dementia who develop delirium are more seriously ill (have required a larger acute insult in order to precipitate delirium) than those with pre-existing brain pathology (dementia). Further research to explain the mortality patterns observed is required in order to translate the findings into clinical care.
Keywords: acute admission; cognition; elderly; function; non-proportional hazards.
Conflict of interest statement
Disclosure PTD reports grants from Shire Pharmaceuticals, Novo Nordisk, and GSK. PTD is a member of the New Drugs Committee of the Scottish Medicines Consortium. The other authors report no conflicts of interest in this work.
Figures
References
-
- Hustey FM, Meldon SW. The prevalence and documentation of impaired mental status in elderly emergency department patients. Ann Emerg Med. 2002;39(3):248–253. - PubMed
-
- Sampson EL, Leurent B, Blanchard MR, Jones L, King M. Survival of people with dementia after unplanned acute hospital admission: a prospective cohort study. Int J Geriatr Psychiatry. 2013;28(10):1015–1022. - PubMed
-
- Li F, Wang F, Jia J. Evaluating the prevalence of dementia in hospitalized older adults and effects of comorbid dementia on patients’ hospital course. Aging Clin Exp Res. 2013;25(4):393–401. - PubMed
-
- Voyer P, Cole MG, McCusker J, Belzile E. Prevalence and symptoms of delirium superimposed on dementia. Clin Nurs Res. 2006;15(1):46–66. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
