

Oxidation-Reduction Potential in Patients undergoing Transcatheter or Surgical Aortic Valve Replacement
- PMID: 30539023
- PMCID: PMC6261068
- DOI: 10.1155/2018/8469383
Oxidation-Reduction Potential in Patients undergoing Transcatheter or Surgical Aortic Valve Replacement
Abstract
Background: Aortic valve stenosis has gained increasingly more importance due to its high prevalence in elderly people. More than two decades ago, transcatheter aortic valve replacement emerged for patients who were denied surgery, and its noninferiority has been demonstrated in numerous studies. Oxidative stress has generated great interest because of its sensitivity to cell damage and the possibility of offering early hints of clinical outcomes. The aim of the present study was to investigate whether there is a significant difference between transcatheter (TAVR) or surgical aortic valve replacement (SAVR) in terms of the changes in oxidation-reduction potential (ORP) and antioxidant capacity. Therefore, we investigated perioperative oxidative stress levels and their influence on clinical outcomes.
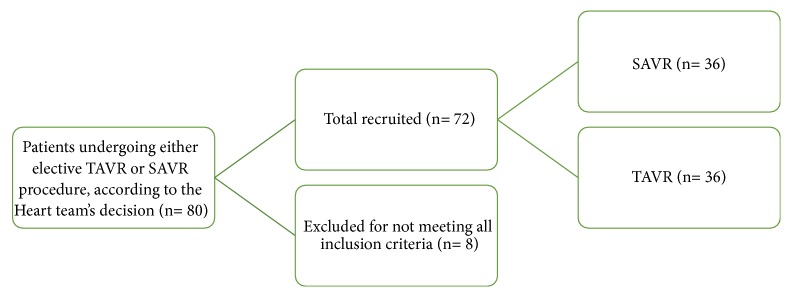
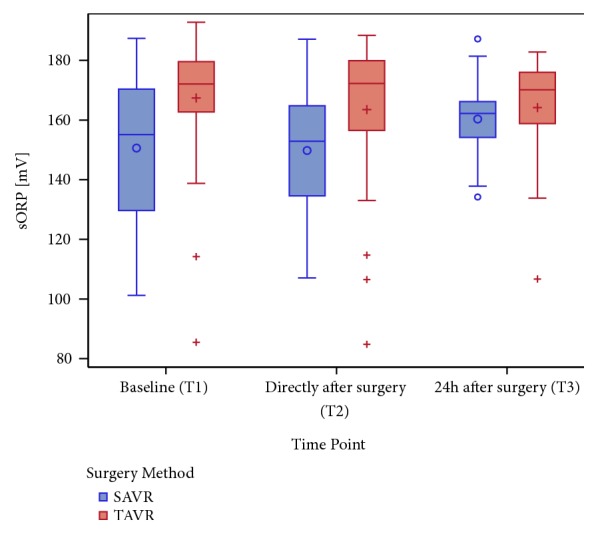
Methods: A total of 72 patients (50% TAVR versus 50% SAVR) were included in the present study. Static oxidation-reduction potential (sORP) and antioxidant capacity were measured using the RedoxSys™ Diagnostic System (Luoxis Diagnostics, USA) in serum samples drawn before and after surgery, as well as on the first postoperative day. In addition, clinical data were obtained to evaluate the clinical outcome of each case.
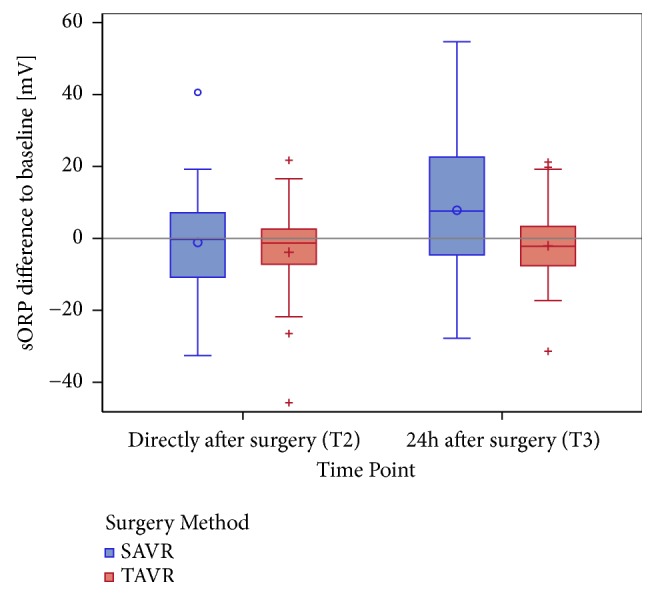
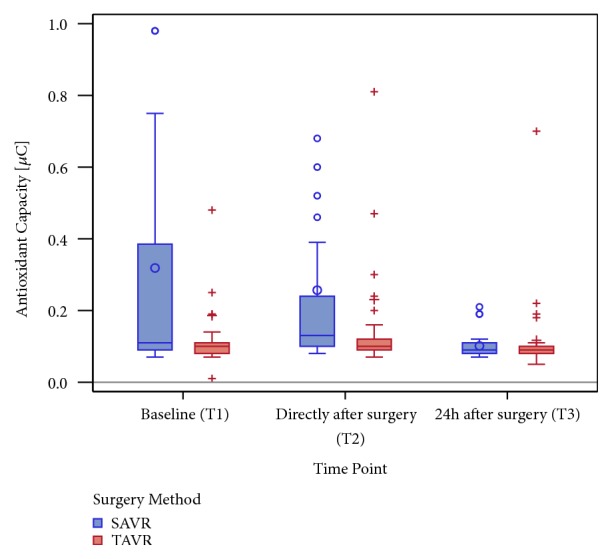
Results: TAVR patients had higher preoperative sORP levels compared to the SAVR patients and more severe comorbidities. Unlike the TAVR cohort, patients in the SAVR group showed a significant difference in sORP from the pre- to postoperative levels. Capacity demonstrated higher preoperative levels in the SAVR cohort and also a greater difference postoperatively compared to the TAVR cohort. Regression analysis revealed a significant correlation between pre- and postoperative capacity levels (r = -0.9931, p < 0.0001), providing a method of predicting postoperative capacity levels by knowing the preoperative levels. According to the multivariable analysis, both sORP and antioxidant capacity are dependent on time point, baseline value, and type of surgery, with the largest variations observed for time effect and surgery method.
Conclusion: A high preoperative sORP level correlated to more severe illness in the TAVR patients. As the TAVR patients did not show significant differences in their preoperative levels, we assume that there was a smaller production of oxidative agents during TAVR due to the less invasive nature of the procedure. Baseline values and development of antioxidant capacity values strengthen this hypothesis. The significant correlation of pre- and postoperative capacity levels might allow high risk patients to be detected more easily and might provide more adequate and individualized therapy preoperatively. This trial is registered with clinicaltrials.gov, identifier: NCT 02488876.
Figures
References
-
- Nishimura R. A., Otto C. M., Bonow R. O. AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017 - PubMed
-
- Nishimura R. A., Otto C. M., Bonow R. O., et al. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(23):2440–2492. doi: 10.1161/CIR.0000000000000029. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
