

SUBCUTANEOUS ONLAY LAPAROSCOPIC APPROACH (SCOLA) FOR VENTRAL HERNIA AND RECTUS ABDOMINIS DIASTASIS REPAIR: TECHNICAL DESCRIPTION AND INITIAL RESULTS
- PMID: 30539974
- PMCID: PMC6284377
- DOI: 10.1590/0102-672020180001e1399
SUBCUTANEOUS ONLAY LAPAROSCOPIC APPROACH (SCOLA) FOR VENTRAL HERNIA AND RECTUS ABDOMINIS DIASTASIS REPAIR: TECHNICAL DESCRIPTION AND INITIAL RESULTS
Abstract
Background: Diastasis of the rectus abdominis muscles (DMRA) is frequent and may be associated with abdominal wall hernias. For patients with redudant skin, dermolipectomy and plication of the diastasis is the most commonly used procedure. However, there is a significant group of patients who do not require skin resection or do not want large incisions.
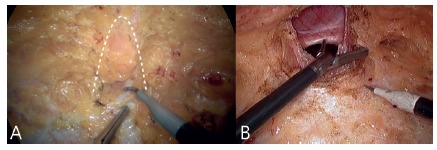
Aim: To describe a "new" technique (subcutaneous onlay laparoscopic approach - SCOLA) for the correction of ventral hernias combined with the DMRA plication and to report the initial results of a case series.
Method: SCOLA was applied in 48 patients to correct ventral hernia concomitant to plication of DMRA by pre-aponeurotic endoscopic technique.
Results: The mean operative time was 93.5 min. There were no intra-operative complications and no conversion. Seroma was the most frequent complication (n=13, 27%). Only one (2%) had surgical wound infection. After a median follow-up of eight months (2-19), only one (2%) patient presented recurrence of DMRA and one (2%) subcutaneous tissue retraction/fibrosis. Forty-five (93.7%) patients reported being satisfied with outcome.
Conclusion: The SCOLA technique is a safe, reproducible and effective alternative for patients with abdominal wall hernia associated with DMRA.
Racional:: A diástase dos músculos retos abdominais (DMRA) é frequente e pode estar associada à presença de hérnias da parede abdominal. Para pacientes com excesso de pele, a dermolipectomia e plicatura da diástase é o procedimento mais comumente utilizado. Entretanto, há um grupo significativo de pacientes que não necessitam ressecção de pele ou não desejam grandes incisões.
Objetivo:: Descrever uma “nova” técnica (Subcutaneous Onlay Laparoscopic Approach - SCOLA) para a correção das hérnias ventrais combinada à plicatura da DMRA e relatar os resultados iniciais.
Métodos:: A técnica SCOLA de correção de hérnia ventral concomitante com a plicatura da DMRA por técnica endoscópica pré-aponeurótica foi aplicada em quarenta e oito pacientes.
Resultados:: O tempo operatório médio foi de 93,5 min. Não houve nenhuma complicação intra-operatória e nenhuma conversão. Seroma foi a complicação mais frequente (n=13, 27%). Apenas um (2%) apresentou infecção de ferida operatória. Após seguimento médio de oito meses (2-19) apenas um (2%) paciente apresentou recidiva da DMRA e um (2%) retração/fibrose do tecido subcutâneo. Quarenta e cinco (93,7%) relataram estarem satisfeitos com resultado.
Conclusão:: A técnica SCOLA é alternativa segura, reprodutível e efetiva para pacientes com hérnia da parede abdominal associada à DMRA.
Conflict of interest statement
Figures





References
-
- American Society of Plastic Surgeons . Plastic surgery statistics report. 2011. http://www.plasticsurgery.org/news-and-resources/ 2012-plastic-surgery-s...
-
- Al Arroyo, Garcia P, Perez F, et al. Randomized clinical trial comparing suture and mesh repair of umbilical hernia in adults. Br J Surg. 2001;88(10):1321–1323. - PubMed
-
- Beer GM, et al. The normal width of the linea alba in nulliparous women. Clin Anat. 2009;22(6):706–711. - PubMed
-
- Bellido Luque J Bellido Luque A, Valdivia J, Suarez Gráu JM, Gomez Menchero J, García Moreno J, Guadalajara Jurado J. Totally endoscopic surgery on diastasis recti associated with midline hernias The advantages of a minimally invasive approach. Prospective cohort study. Hernia. 2015;19(3):493–501. - PubMed
-
- Belyansky I, Daes J, Radu VG, Balasubramanian R, Reza Zahiri H, Weltz AS, Sibia US, Park A, Novitsky Y. A novel approach using the enhanced-view totally extraperitoneal (eTEP) technique for laparoscopic retromuscular hernia repair. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
