

Surgical treatment of gastric cancer: a 10-year experience in a high-volume university hospital
- PMID: 30540120
- PMCID: PMC6256993
- DOI: 10.6061/clinics/2018/e543s
Surgical treatment of gastric cancer: a 10-year experience in a high-volume university hospital
Abstract
Objectives: Surgery remains the cornerstone treatment modality for gastric cancer, the fifth most common type of tumor in Brazil. The aim of this study was to analyze the surgical treatment outcomes of patients with gastric cancer who were referred to a high-volume university hospital.
Methods: We reviewed all consecutive patients who underwent any surgical procedure due to gastric cancer from a prospectively collected database. Clinicopathological characteristics, surgical and survival outcomes were evaluated, with emphasis on patients treated with curative intent.
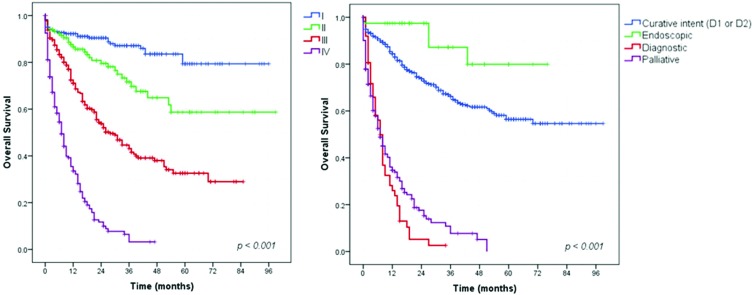
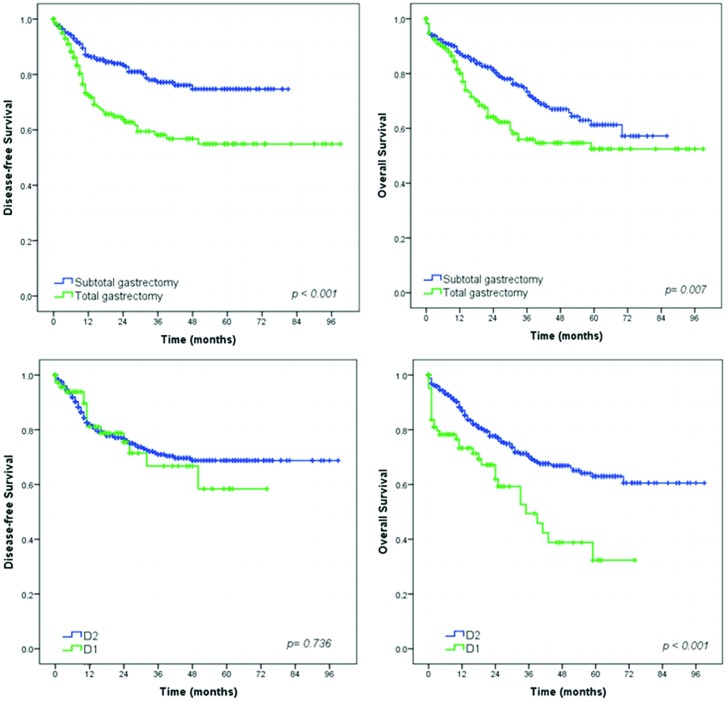
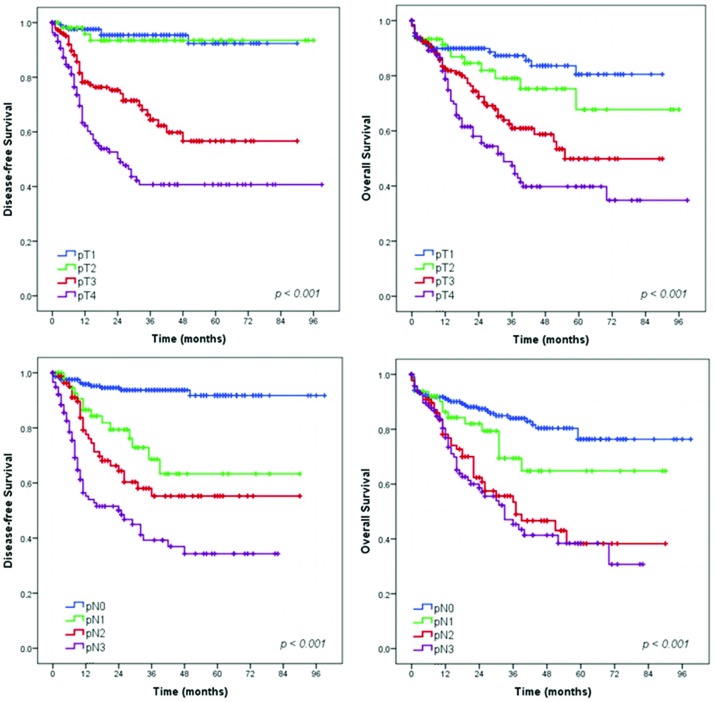
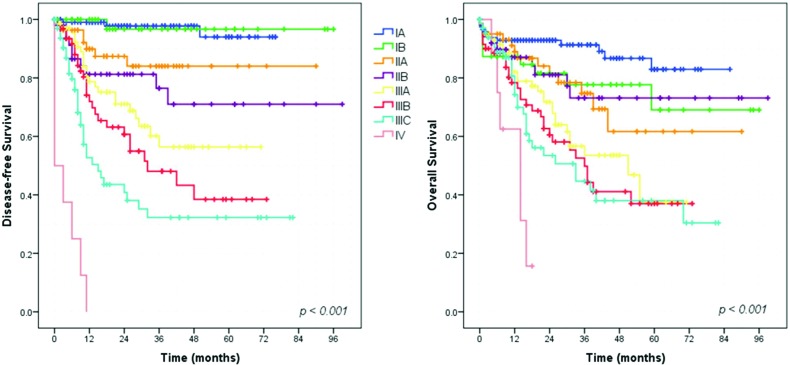
Results: From 2008 to 2017, 934 patients with gastric tumors underwent surgical procedures in our center. Gastric adenocarcinoma accounted for the majority of cases. Of the 875 patients with gastric adenocarcinoma, resection with curative intent was performed in 63.5%, and palliative treatment was performed in 22.4%. The postoperative surgical mortality rate for resected cases was 5.3% and was related to D1 lymphadenectomy and the presence of comorbidities. Analysis of patients treated with curative intent showed that resection extent, pT category, pN category and final pTNM stage were related to disease-free survival (DFS) and overall survival (OS). The DFS rates for D1 and D2 lymphadenectomy were similar, but D2 lymphadenectomy significantly improved the OS rate. Additionally, clinical factors and the presence of comorbidities had influence on the OS.
Conclusions: TNM stage and the type of lymphadenectomy were independent factors related to prognosis. Early diagnosis should be sought to offer the optimal surgical approach in patients with less-advanced disease.
Figures
References
-
- Instituto Nacional de Câncer José Alencar Gomes da Silva (INCA) Estimativa 2016: incidência de câncer no Brasil. Rio de Janeiro (RJ): INCA; 2015.
-
- Bosman TF, Carneiro F, Hruban RH, Theise ND. WHO Classification of Tumours of the Digestive System. 4th ed. Lyon: International Agency for Research on cancer (IARC) Press; 2010.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
