

Effects of vasodilating medications on cerebral haemodynamics in health and disease: systematic review and meta-analysis
- PMID: 30540658
- PMCID: PMC6513078
- DOI: 10.1097/HJH.0000000000002033
Effects of vasodilating medications on cerebral haemodynamics in health and disease: systematic review and meta-analysis
Abstract
Objectives: Vasodilating antihypertensives prevent stroke and potentially cerebral small vessel disease but their effects on cerebrovascular haemodynamics beyond blood pressure lowering are unclear.
Methods: We searched PubMed, Medline, Embase, Cinahl, Psychinfo, Health Business Elite and Health Management Information Consortium for randomized studies of vasodilating medications, compared to no treatment or nonvasodilators, that reported effects on cerebral blood flow (CBF), mean blood flow velocity (MFV) or cerebrovascular reactivity. Absolute and standardized mean differences (SMD) were combined by inverse-variance weighted fixed or random-effects meta-analysis stratified by study design, population characteristics and vasodilator class.
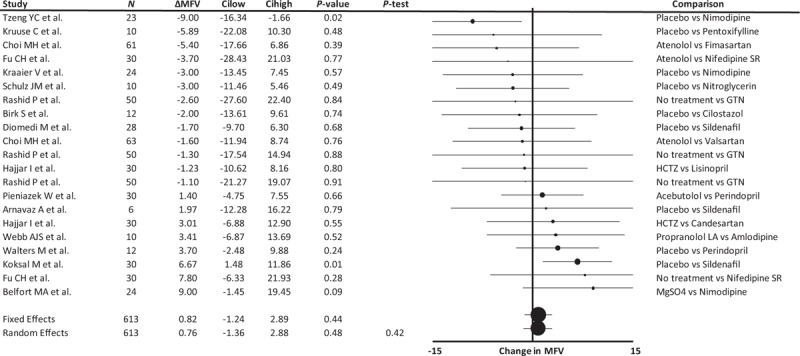
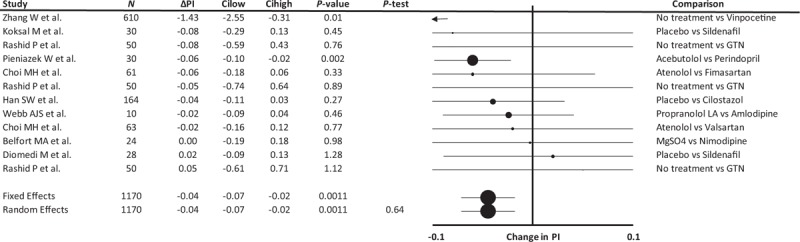
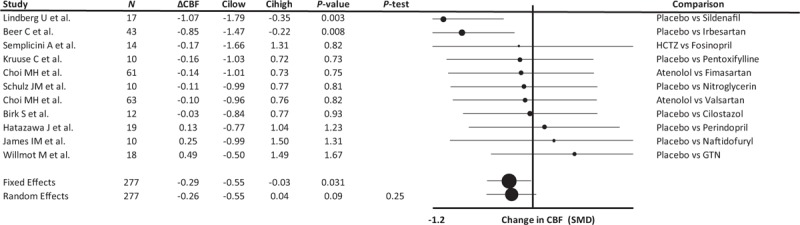
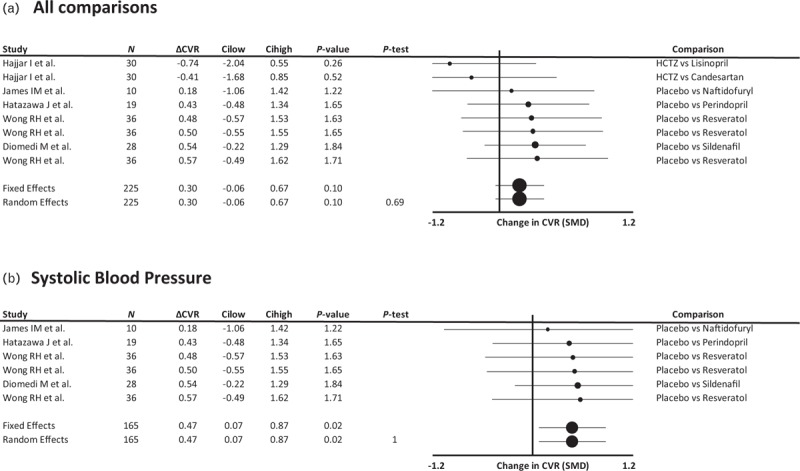
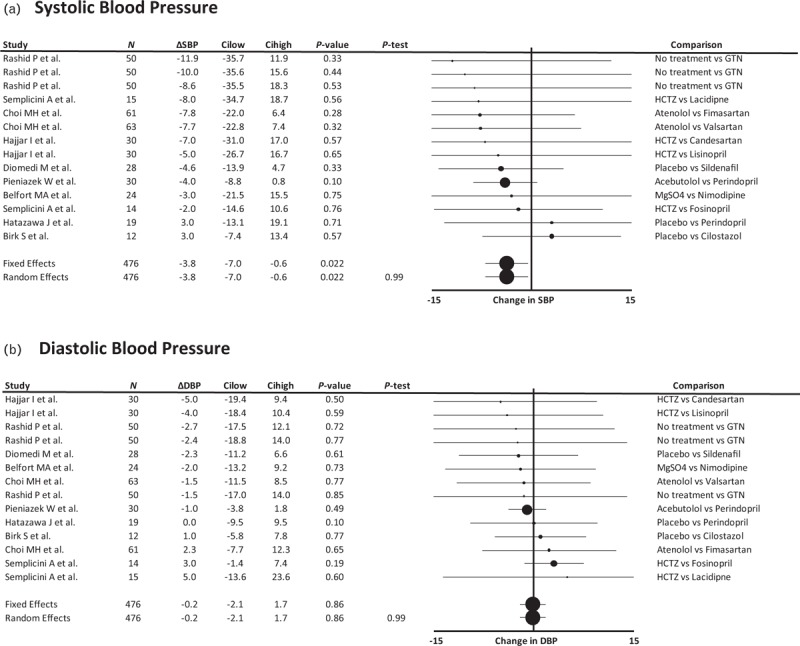
Results: In 35 studies reporting 57 comparisons, there was a reduction in SBP (-4.13 mmHg, -7.55 to -0.71, P = 0.018) but no change in MFV (ΔMFV 1.11, confidence interval -0.93 to 3.14, P = 0.29, 23 comparisons). MFV increased in patients with underlying conditions (3.41, 0.24 to 6.57, P = 0.04) but not in healthy study participants (-1.27, -5.18 to 2.64, P = 0.68), with no differences by vasodilating drug class. Cerebral pulsatility index was reduced across all studies (Δ pulsatility index -0.04, -0.07 to -0.02, P = 0.001; Δ pulsatility index -SMD -0.32, -0.47 to -0.16, P < 0.001), except in studies reporting responses to single drug doses (Δ pulsatility index 0.00, -0.09 to -0.08, P = 0.93). Despite evidence of reporting and publication bias, there was an apparent consistent reduction in CBF with vasodilators (CBF-SMD -0.24, -0.46 to -0.02, P = 0.03) with a significant increase in cerebrovascular reactivity-SMD (0.48, 0.13-0.83, P = 0.007).
Conclusions: Despite reducing SBP, vasodilators did not significantly impair absolute CBF but improved cerebrovascular pulsatility and reactivity, suggesting therapeutic potential in preventing stroke and cerebral small vessel disease.
Figures
References
-
- Webb AJ, Fischer U, Mehta Z, Rothwell PM. Effects of antihypertensive-drug class on interindividual variation in blood pressure and risk of stroke: a systematic review and meta-analysis. Lancet 2010; 375:906–915. - PubMed
-
- Dufouil C, Chalmers J, Coskun O, Besancon V, Bousser MG, Guillon P, et al. Effects of blood pressure lowering on cerebral white matter hyperintensities in patients with stroke: the PROGRESS (Perindopril Protection Against Recurrent Stroke Study) Magnetic Resonance Imaging Substudy. Circulation 2005; 112:1644–1650. - PubMed
-
- Rothwell PM, Howard SC, Dolan E, O’Brien E, Dobson JE, Dahlof B, et al. Effects of beta blockers and calcium-channel blockers on within-individual variability in blood pressure and risk of stroke. Lancet Neurol 2010; 9:469–480. - PubMed
-
- Webb AJ, Fischer U, Rothwell PM. Effects of beta-blocker selectivity on blood pressure variability and stroke: a systematic review. Neurology 2011; 77:731–737. - PubMed
-
- Shinohara Y, Katayama Y, Uchiyama S, Yamaguchi T, Handa S, Matsuoka K, et al. Cilostazol for prevention of secondary stroke (CSPS 2): an aspirin-controlled, double-blind, randomised noninferiority trial. Lancet Neurol 2010; 9:959–968. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
