

Relationship between plaque composition by virtual histology intravascular ultrasound and clinical outcomes after percutaneous coronary intervention in saphenous vein graft disease patients: study protocol of a prospective cohort study
- PMID: 30541457
- PMCID: PMC6291998
- DOI: 10.1186/s12872-018-0975-1
Relationship between plaque composition by virtual histology intravascular ultrasound and clinical outcomes after percutaneous coronary intervention in saphenous vein graft disease patients: study protocol of a prospective cohort study
Abstract
Background: Plaque composition and morphologic characteristics identified by virtual histology intravascular ultrasound (VH-IVUS) can determine plaques at increased risk of clinical events following percutaneous coronary intervention (PCI) among coronary artery disease (CAD) patients. However, there have been few studies to investigate the relationship between plaque composition of saphenous vein graft (SVG) by VH-IVUS and clinical outcomes in patients with saphenous vein graft disease (SVGD) undergoing PCI. The purpose of this study is to determine whether plaque components and characteristics by VH-IVUS can predict major adverse cardiac events (MACEs) among SVGD patients undergoing PCI.
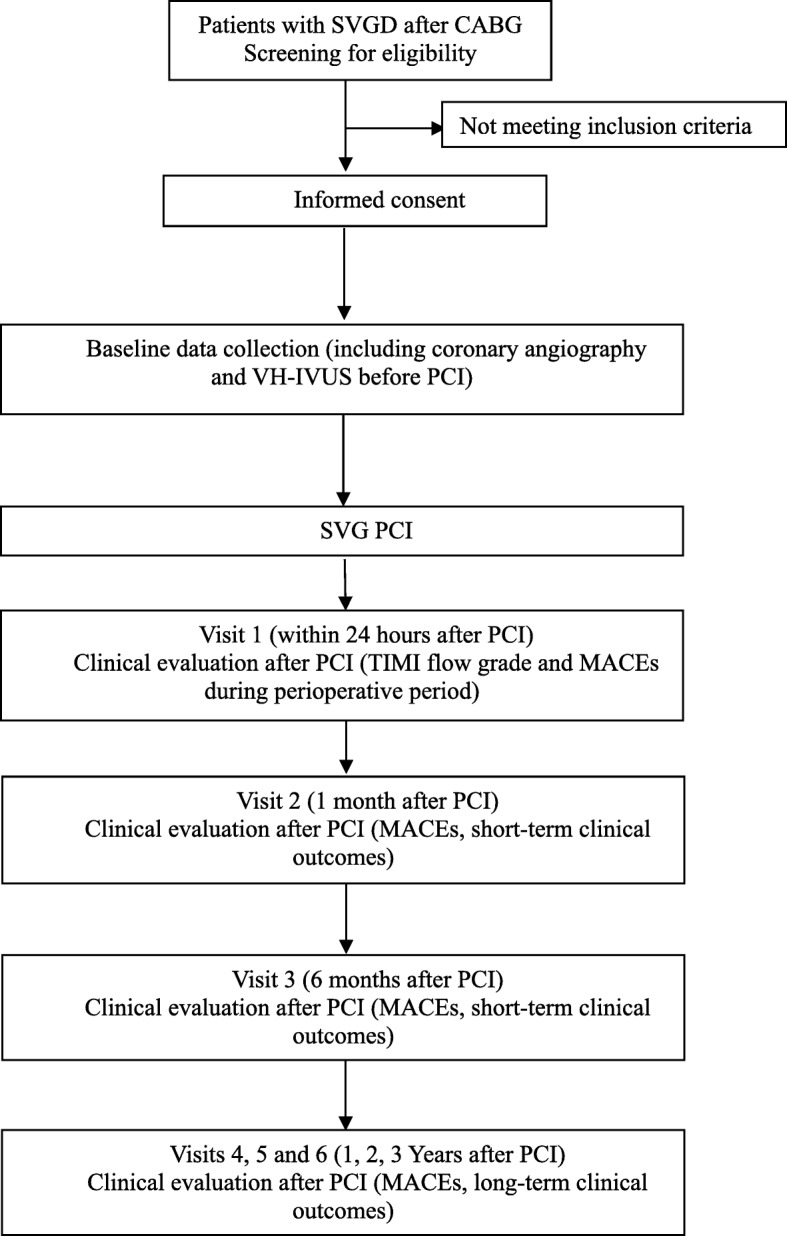
Methods/design: This is a prospective cohort study conducted in Tianjin Chest Hospital, China. Participants with SVGD referred for PCI will be invited to participate in this study, and will be followed up at 1, 6, 12, 24 and 36 months post-PCI to assess clinical outcomes. The planned sample size is 175 subjects. We will recruit subjects with SVGD scheduled to receive PCI, aged 18-80 years, with a history of previous coronary artery bypass graft (CABG) surgery more than 1 year ago, and willing to participate in the study and sign informed consent. The composite primary study endpoint is the incidence of MACEs after PCI for SVGD, including death from cardiac causes, non-fatal myocardial infarction, unplanned target lesion revascularization (TLR) and target vessel revascularization (TVR). The primary outcome analysis will be presented as Kaplan-Meier estimates and the primary outcome analysis will be carried out using a Cox proportional hazards regression model.
Discussion: Once the predictive values of plaque components and characteristics by VH-IVUS on subsequent clinical outcomes are determined among SVGD patients undergoing PCI, an innovative prediction tool of clinical outcomes for SVGD patients undergoing PCI will be created, which may lead to the development of new methods of risk stratification and intervention guidance.
Trial registration: The study is registered to ClinicalTrials.gov (NCT03175952).
Keywords: Major adverse cardiac events; Percutaneous coronary intervention; Saphenous vein graft disease; Virtual histology intravascular ultrasound.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol has been approved by the Institutional Review Boards of Tianjin Chest Hospital and the study will be conducted in accordance with Declaration of Helsinki. Written informed consent is signed by all the participants. The study is also registered at
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Similar articles
-
Application of virtual histological intravascular ultrasound in plaque composition assessment of saphenous vein graft diseases.Chin Med J (Engl). 2019 Apr 20;132(8):957-962. doi: 10.1097/CM9.0000000000000183. Chin Med J (Engl). 2019. PMID: 30958438 Free PMC article.
-
Prediction of Major Adverse Cardiovascular Events and Slow/No-Reflow by Virtual Histology Imaging After Percutaneous Interventions on Saphenous Vein Grafts.Angiology. 2020 Mar;71(3):263-273. doi: 10.1177/0003319719892354. Epub 2019 Dec 23. Angiology. 2020. PMID: 31867979
-
Percutaneous Coronary Intervention of Saphenous Vein Graft.Circ Cardiovasc Interv. 2017 May;10(5):e004953. doi: 10.1161/CIRCINTERVENTIONS.117.004953. Circ Cardiovasc Interv. 2017. PMID: 28495896
-
Drug eluting versus bare metal stents for percutaneous coronary intervention of saphenous vein graft lesions: An updated meta-analysis of randomized controlled trials.Cardiovasc Revasc Med. 2018 Oct-Nov;19(7 Pt B):837-844. doi: 10.1016/j.carrev.2018.03.025. Epub 2018 Apr 3. Cardiovasc Revasc Med. 2018. PMID: 29685385
-
Drug-Eluting Stents Versus Bare-Metal Stents in Saphenous Vein Graft Intervention.Circ Cardiovasc Interv. 2018 Nov;11(11):e007045. doi: 10.1161/CIRCINTERVENTIONS.118.007045. Circ Cardiovasc Interv. 2018. PMID: 30571204
References
-
- Gaudino M, Puskas JD, Di Franco A, Ohmes LB, Iannaccone M, Barbero U, Glineur D, Grau JB, Benedetto U, D'Ascenzo F, et al. Three arterial grafts improve late survival: a meta-analysis of propensity-matched studies. Circulation. 2017;135(11):1036–1044. doi: 10.1161/CIRCULATIONAHA.116.025453. - DOI - PubMed
-
- Barbero U, Iannaccone M, d’Ascenzo F, Barbero C, Mohamed A, Annone U, Benedetto S, Celentani D, Gagliardi M, Moretti C, et al. 64 slice-coronary computed tomography sensitivity and specificity in the evaluation of coronary artery bypass graft stenosis: a meta-analysis. Int J Cardiol. 2016;216:52–57. doi: 10.1016/j.ijcard.2016.04.156. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
