

Safety and effectiveness of antimalarial therapy in sickle cell disease: a systematic review and network meta-analysis
- PMID: 30541465
- PMCID: PMC6292161
- DOI: 10.1186/s12879-018-3556-0
Safety and effectiveness of antimalarial therapy in sickle cell disease: a systematic review and network meta-analysis
Abstract
Background: About 80% of all reported sickle cell disease (SCD) cases in children anually are recorded in Africa. Although malaria is considered a major cause of death in SCD children, there is limited data on the safety and effectiveness of the available antimalarial drugs used for prophylaxis. Also, previous systematic reviews have not provided quantitative measures of preventive effectiveness. The purpose of this research was to conduct a systematic review and meta-analysis of the available literature to determine the safety and effectiveness of antimalarial chemoprophylaxis used in SCD patients.
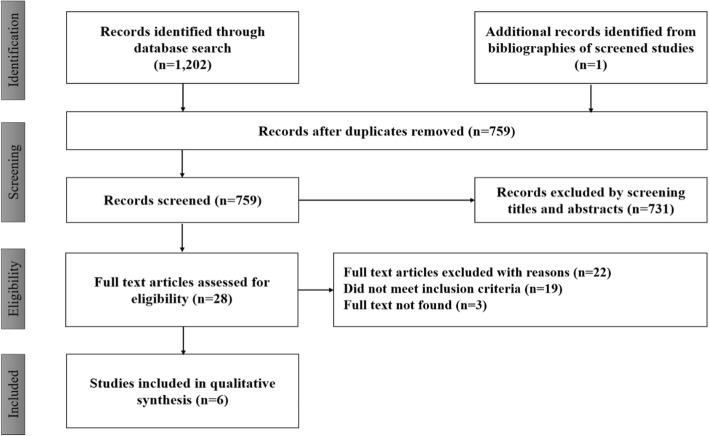
Methods: We searched in PubMed, Medline, CINAHL, POPLine and Cochrane library, for the period spanning January 1990 to April 2018. We considered randomized or quasi-randomized controlled trials comparing any antimalarial chemoprophylaxis to, 1) other antimalarial chemoprophylaxis, 2) placebo or 3) no intervention, in SCD patients. Studies comparing at least two treatment arms, for a minimum duration of three months, with no restriction on the number of patients per arm were reviewed. The data were extracted and expressed as odds ratios. Direct pairwise comparisons were performed using fixed effect models and the heterogeneity assessed using the I-square.
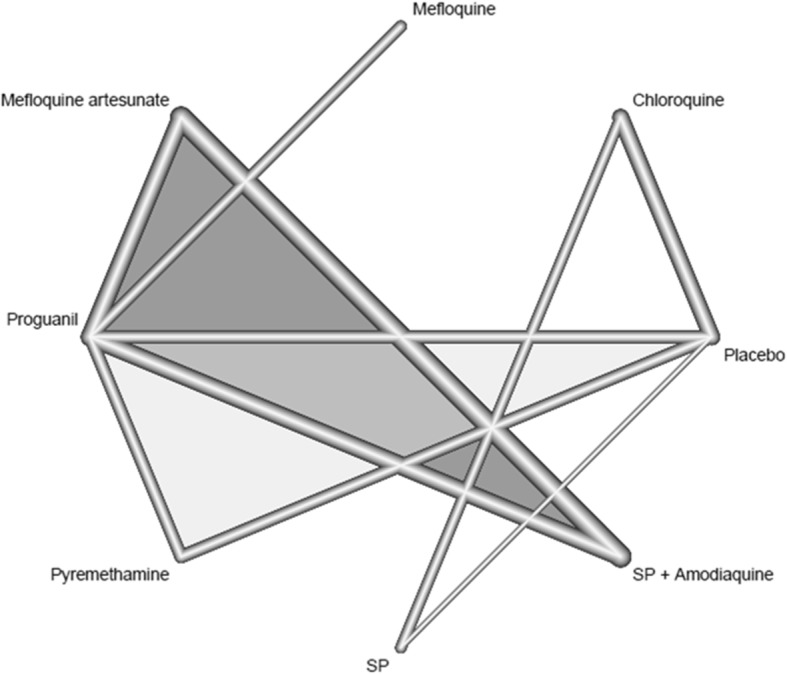
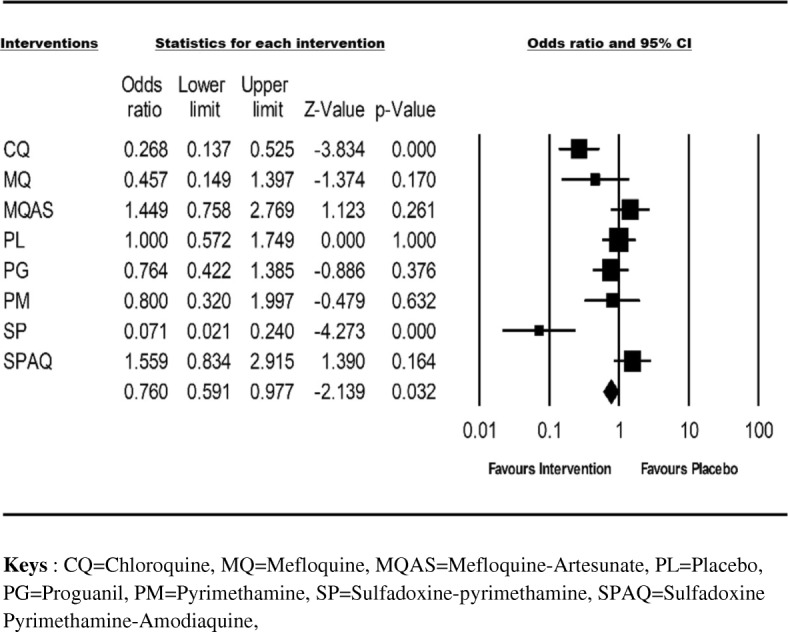
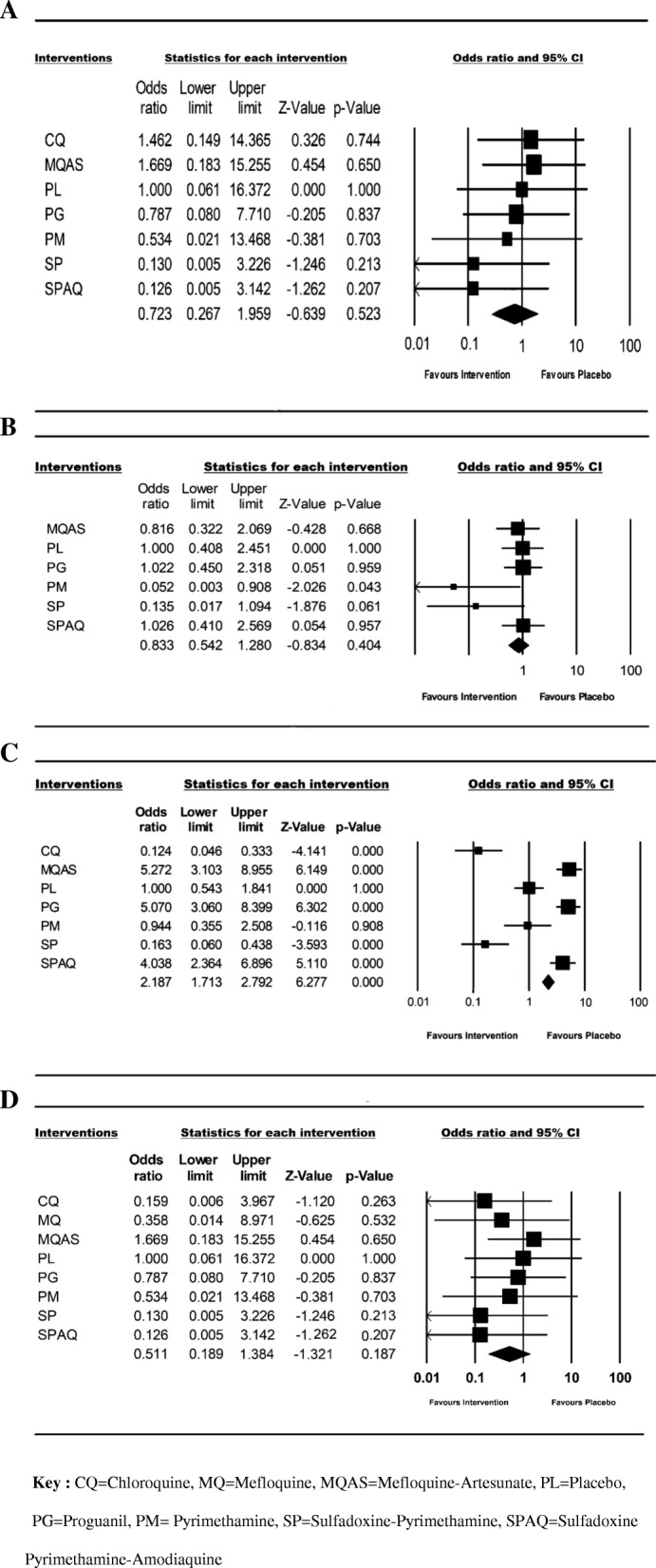
Results: Six qualified studies that highlighted the importance of antimalarial chemoprophylaxis in SCD children were identified. In total, seven different interventions (Chloroquine, Mefloquine, Mefloquine artesunate, Proguanil, Pyrimethamine, Sulfadoxine-pyrimethamine, Sulfadoxine-pyrimethamine amodiaquine) were evaluated in 912 children with SCD. Overall, the meta-analysis showed that antimalarial chemoprophylaxis provided protection against parasitemia and clinical malaria episodes in children with SCD. Nevertheless, the risk of hospitalization (OR = 0.72, 95% CI = 0.267-1.959; I2 = 0.0%), blood transfusion (OR = 0.83, 95% CI = 0.542-1.280; I2 = 29.733%), vaso-occlusive crisis (OR = 19, 95% CI = 1.713-2.792; I2 = 93.637%), and mortality (OR = 0.511, 95% CI = 0.189-1.384; I2 = 0.0%) did not differ between the intervention and placebo groups.
Conclusion: The data shows that antimalarial prophylaxis reduces the incidence of clinical malaria in children with SCD. However, there was no difference between the occurrence of adverse events in children who received placebo and those who received prophylaxis. This creates an urgent need to assess the efficacy of new antimalarial drug regimens as potential prophylactic agents in SCD patients.
Systematic review registration: PROSPERO (CRD42016052514).
Keywords: Adverse events; Chemoprophylaxis; Effectiveness; Malaria; Safety; Sickle cell disease.
Conflict of interest statement
Authors’ information
AF and LGT are supported by a Ph.D. fellowship from a World Bank African Centres of Excellence Grant (ACE02-WACCBIP: Awandare); AF is also supported by the International Development Research Center grant from the African Institute for Mathematical Sciences, Ghana, a recipient of the L’Oreal-UNESCO for Women in Science Grant, the Carnegie Corporation of New York and the University of Ghana BanGA Ph.D. Grant.
Ethics approval and consent to participate
Not applicable.
Consent for publication
The authors have read and agreed to the content of this manuscript and its publication upon acceptance.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Monthly sulphadoxine-pyrimethamine combination versus daily proguanil for malaria chemoprophylaxis in sickle cell disease: a randomized controlled study at the Jos University Teaching Hospital.Niger J Med. 2016 Apr-Jun;25(2):119-27. Niger J Med. 2016. PMID: 29944308 Clinical Trial.
-
Mefloquine for preventing malaria in pregnant women.Cochrane Database Syst Rev. 2018 Nov 14;11(11):CD011444. doi: 10.1002/14651858.CD011444.pub3. Cochrane Database Syst Rev. 2018. PMID: 30480761 Free PMC article.
-
A Randomized Trial to Compare the Safety, Tolerability, and Effectiveness of 3 Antimalarial Regimens for the Prevention of Malaria in Nigerian Patients With Sickle Cell Disease.J Infect Dis. 2015 Aug 15;212(4):617-25. doi: 10.1093/infdis/jiv093. Epub 2015 Feb 20. J Infect Dis. 2015. PMID: 25701866 Free PMC article. Clinical Trial.
-
Malaria chemoprophylaxis in sickle cell disease.Cochrane Database Syst Rev. 2019 Nov 4;2019(11). doi: 10.1002/14651858.CD003489.pub2. Cochrane Database Syst Rev. 2019. PMID: 31681984
-
Monthly sulfadoxine/pyrimethamine-amodiaquine or dihydroartemisinin-piperaquine as malaria chemoprevention in young Kenyan children with sickle cell anemia: A randomized controlled trial.PLoS Med. 2022 Oct 10;19(10):e1004104. doi: 10.1371/journal.pmed.1004104. eCollection 2022 Oct. PLoS Med. 2022. PMID: 36215323 Free PMC article. Clinical Trial.
Cited by
-
Beyond Childhood: Adult and Adolescent Sickle Cell Disease and Outcomes in Northern Ghana.EJHaem. 2025 Mar 21;6(2):e70023. doi: 10.1002/jha2.70023. eCollection 2025 Apr. EJHaem. 2025. PMID: 40123794 Free PMC article.
-
Treatment Options That Reduce the Duration of Sickle Cell Vaso-Occlusive Crises: A Systematic Review.Cureus. 2022 Aug 24;14(8):e28337. doi: 10.7759/cureus.28337. eCollection 2022 Aug. Cureus. 2022. PMID: 36176876 Free PMC article. Review.
-
Sickle Cell Disease in Children and Adolescents: A Review of the Historical, Clinical, and Public Health Perspective of Sub-Saharan Africa and Beyond.Int J Pediatr. 2022 Oct 8;2022:3885979. doi: 10.1155/2022/3885979. eCollection 2022. Int J Pediatr. 2022. PMID: 36254264 Free PMC article. Review.
-
Indications for hospitalisation and predictors of 30-day re-admission of patients with sickle cell disease in Uganda: a retrospective study.BMJ Open. 2025 Aug 8;15(8):e104303. doi: 10.1136/bmjopen-2025-104303. BMJ Open. 2025. PMID: 40780722 Free PMC article.
-
Improvement of SCD morbimortality in children: experience in a remote area of an African country.BMC Health Serv Res. 2021 Apr 1;21(1):294. doi: 10.1186/s12913-021-06286-7. BMC Health Serv Res. 2021. PMID: 33794895 Free PMC article.
References
-
- WHO. Sickle-cell anaemia. In. Edited by A59/9. R. Geneva: WHO; 2006.
-
- Diallo DA, Baby M, Boire A, Diallo YL. Management of pain of acute sickle cell pain crises by health care providers in Mali. Med Trop (Mars) 2008;68(5):502–506. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
