

Aspergillus pseudodeflectus: a new human pathogen in liver transplant patients
- PMID: 30541477
- PMCID: PMC6292062
- DOI: 10.1186/s12879-018-3527-5
Aspergillus pseudodeflectus: a new human pathogen in liver transplant patients
Abstract
Background: Liver transplant recipients are at high risk of developing invasive aspergillosis and in particular by Aspergillus fumigatus which is the most commonly encountered species in this population. Other non-fumigatus Aspergillus species with reduced susceptibility to antifungal drugs can also be involved. Accurate identification associated to antifungal susceptibility testing is essential for therapy adjustment. We report a case of invasive pulmonary aspergillosis due to Aspergillus pseudodeflectus in a liver transplant recipient. To our knowledge, this is the first reported case of invasive aspergillosis due to this species with a reduced susceptibility to azoles.
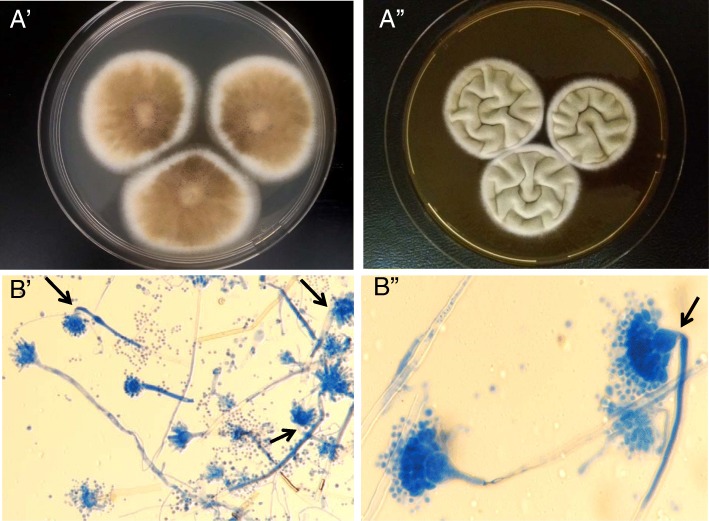
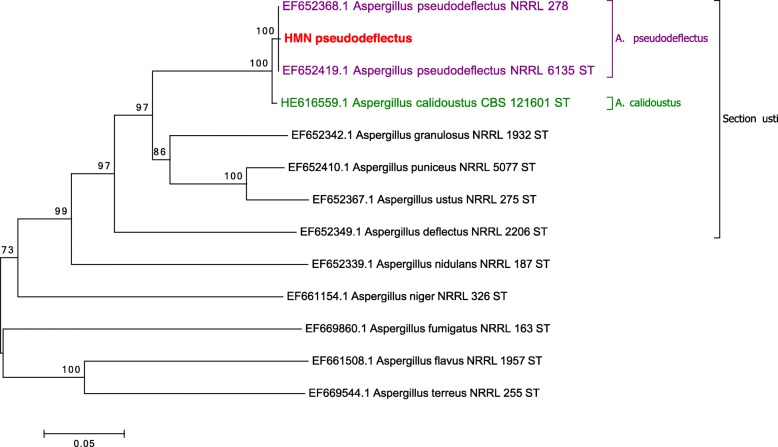
Case presentation: A 64 year-old woman with drug-induced fulminant hepatitis underwent liver transplantation. Prophylactic treatment with caspofungin was introduced due to aspergillosis risk factors consisting in hemodialysis and fulminant hepatitis. Six weeks after transplantation, CT scan showed a right pulmonary opacity associated with an increase of galactomannan (index 5.4). Culture of BAL grew with several colonies of Aspergillus sp. The diagnosis of invasive aspergillosis was probable according to the EORTC criteria. The antifungal susceptibility tests (Etest®) revealed low MICs to echinocandins and amphotericin B) but high MICs to azoles. After these results, voriconazole was switched to liposomal amphotericin B. The patient died one month after diagnosis from a refractory septic shock with multiple organ failure. A molecular identification of isolate, based on partial β-tubulin and calmodulin genes, was performed and identified A. pseudodeflectus.
Conclusions: Our case raises the question of pathogenicity of this species, which belongs to Aspergillus section Usti and is genetically and morphologically very close to Aspergillus calidoustus that was previously reported in human transplant recipients.
Keywords: Aspergillosis; Aspergillus pseudodeflectus; Azoles resistance; Liver transplantation; Molecular identification.
Conflict of interest statement
Ethics approval and consent to participate
This study was carried out in compliance with the Helsinki declaration. All liver transplants of our institution have read and approved the hospital welcome book, which states that their biological samples, after use, may be used for publication in the context of biological collections (except for genetic analyzes). Henri Mondor ethical committee approved the study protocol and database has been declared to the Commission Nationale de l’Informatique et des Libertés (CNIL) (n°1,699,340).
Consent for publication
Written informed consent was obtained from the patient’s family for the publication of this manuscript. No images or videos relating to the individual person were included in this article.
Competing interests
ED has received grants from Gilead, Ferrer, and Biorad, and payment for lectures from Gilead, MSD, and Schering. ED has also been a consultant for Astellas and Innothera. FB received grants from Astellas, and payment for lectures from Merck. NAA, EL, JBM, SI, FF, declare no conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Invasive pulmonary aspergillosis due to Aspergillus lentulus: Successful treatment of a liver transplant patient.J Infect Chemother. 2015 Jun;21(6):479-81. doi: 10.1016/j.jiac.2015.02.010. Epub 2015 Mar 6. J Infect Chemother. 2015. PMID: 25828927
-
Invasive aspergillosis caused by cryptic species in transplant recipients: A review.Med Mycol. 2025 Jan 25;63(2):myaf015. doi: 10.1093/mmy/myaf015. Med Mycol. 2025. PMID: 39933579 Review.
-
Invasive aspergillosis in liver transplant recipients.Transpl Infect Dis. 2023 Jun;25(3):e14049. doi: 10.1111/tid.14049. Epub 2023 Mar 16. Transpl Infect Dis. 2023. PMID: 36929539 Review.
-
Proven Invasive Pulmonary Aspergillosis in Stem Cell Transplant Recipient Due to Aspergillus sublatus, a Cryptic Species of A. nidulans.Mycopathologia. 2018 Apr;183(2):423-429. doi: 10.1007/s11046-017-0223-8. Epub 2017 Nov 11. Mycopathologia. 2018. PMID: 29128933
-
Changes in In Vitro Susceptibility Patterns of Aspergillus to Triazoles and Correlation With Aspergillosis Outcome in a Tertiary Care Cancer Center, 1999-2015.Clin Infect Dis. 2017 Jul 15;65(2):216-225. doi: 10.1093/cid/cix297. Clin Infect Dis. 2017. PMID: 28379304 Free PMC article.
Cited by
-
Clinical Relevance and Characteristics of Aspergillus calidoustus and Other Aspergillus Species of Section Usti.J Fungi (Basel). 2020 Jun 12;6(2):84. doi: 10.3390/jof6020084. J Fungi (Basel). 2020. PMID: 32545485 Free PMC article. Review.
-
Fungal Infections in Liver Transplant Recipients.J Fungi (Basel). 2021 Jun 29;7(7):524. doi: 10.3390/jof7070524. J Fungi (Basel). 2021. PMID: 34210106 Free PMC article. Review.
-
A Practical Workflow for the Identification of Aspergillus, Fusarium, Mucorales by MALDI-TOF MS: Database, Medium, and Incubation Optimization.J Clin Microbiol. 2022 Dec 21;60(12):e0103222. doi: 10.1128/jcm.01032-22. Epub 2022 Nov 3. J Clin Microbiol. 2022. PMID: 36326257 Free PMC article.
References
-
- Singh N, Husain S. The AST infectious diseases Community of Practice. Invasive aspergillosis in solid organ transplant recipients. Am J Transplant. 2009;9:S180–S191. - PubMed
-
- Neofytos D, Treadway S, Ostrander D, Alonso CD, Dierberg KL, Nussenblatt V, et al. Epidemiology, outcomes, and mortality predictors of invasive mold infections among transplant recipients: a 10-year, single-center experience. Transpl Infect Dis Off J Transplant Soc. 2013;15(3):233–242. - PMC - PubMed
-
- Barchiesi F, Mazzocato S, Mazzanti S, Gesuita R, Skrami E, Fiorentini A, et al. Invasive aspergillosis in liver transplant recipients: epidemiology, clinical characteristics, treatment, and outcomes in 116 cases. Liver Transpl. 2015;21(2):204–212. - PubMed
-
- Walter J, Sobottka I, Rogiers X, Broering D, Fischer L. Invasive aspergillosis caused by aspergillus terreus in a living donor liver transplant recipient successfully treated by caspofungin. Mycoses. 2011;54(4):e220–e222. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
