

Simultaneous bilateral posterior ischemic optic neuropathy secondary to giant cell arteritis: a case presentation and review of the literature
- PMID: 30541489
- PMCID: PMC6292061
- DOI: 10.1186/s12886-018-0994-9
Simultaneous bilateral posterior ischemic optic neuropathy secondary to giant cell arteritis: a case presentation and review of the literature
Abstract
Background: This report highlights a rare case of simultaneous bilateral blindness due to posterior ischemic optic neuropathy. Typically, ophthalmic involvement in giant cell arteritis is monocular or sequential ischemia of the anterior portion of the optic nerve, and less frequently simultaneous.
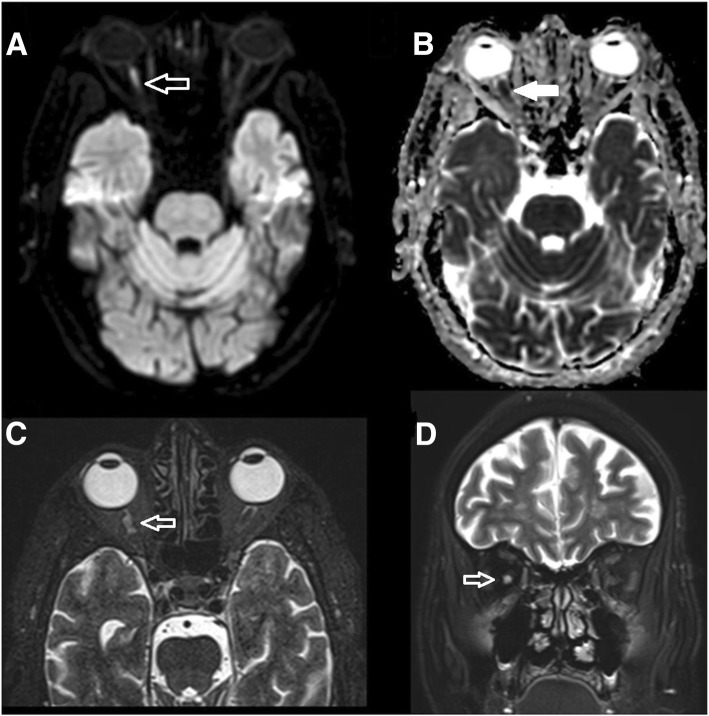
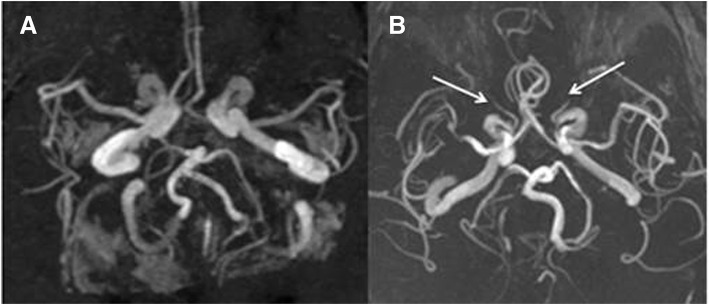
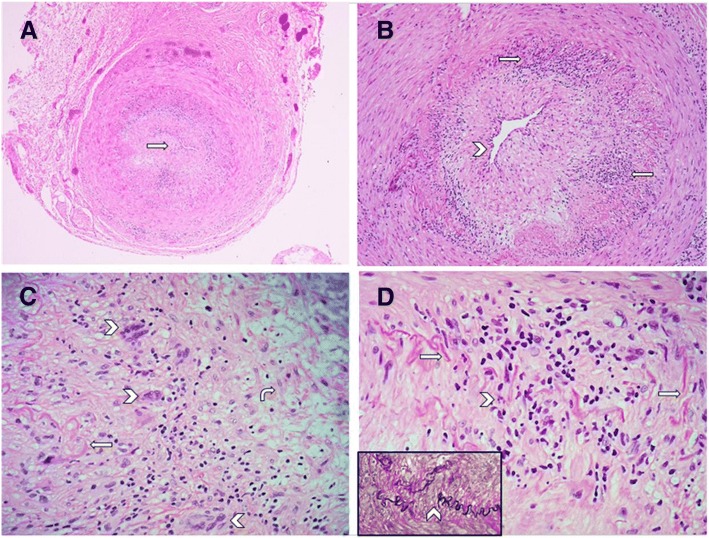
Case presentation: An 80-year-old Saudi male came with a history of simultaneous bilateral vision loss 5 days prior to presentation. The exam showed dilated non-reactive pupils, no light perception in both eyes, and normal fundus exam. C-reactive protein and erythrocyte sedimentation rate levels were high Magnetic resonance imaging and magnetic resonance angiography of the brain showed a right posterior optic nerve lesion and absence of flow in both ophthalmic arteries respectively. A left temporal artery biopsy confirmed giant cell arteritis.
Conclusion: The presentation of GCA can be atypical and patients may present with simultaneous blindness. Bilateral simultaneous PION does not exclusively occur in a post surgical setting, emphasizing the importance of decreasing the threshold of suspicion of similar cases to avoid further neurological complications.
Keywords: Blindness; Giant cell arteritis; Headache; Neuro-ophthalmology; Posterior ischemic optic neuropathy.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the consent form is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Giant cell arteritis presenting as bilateral anterior ischemic optic neuropathy: a biopsy-proven case report in Chinese patient.BMC Ophthalmol. 2018 Oct 30;18(1):282. doi: 10.1186/s12886-018-0953-5. BMC Ophthalmol. 2018. PMID: 30376812 Free PMC article.
-
[Bilateral amaurosis in 11 patients with giant cell arteritis confirmed by arterial biopsy].Klin Monbl Augenheilkd. 2001 Oct;218(10):658-61. doi: 10.1055/s-2001-18387. Klin Monbl Augenheilkd. 2001. PMID: 11706381 German.
-
Three-Dimensional High-Resolution Black-Blood Magnetic Resonance Imaging for Detection of Arteritic Anterior Ischemic Optic Neuropathy in Patients With Giant Cell Arteritis.Invest Radiol. 2018 Nov;53(11):698-704. doi: 10.1097/RLI.0000000000000500. Invest Radiol. 2018. PMID: 30095558
-
Giant cell arteritis: ophthalmic manifestations of a systemic disease.Graefes Arch Clin Exp Ophthalmol. 2016 Dec;254(12):2291-2306. doi: 10.1007/s00417-016-3434-7. Epub 2016 Aug 5. Graefes Arch Clin Exp Ophthalmol. 2016. PMID: 27495301 Review.
-
Arteritic anterior ischaemic optic neuropathy: An update.Eur J Ophthalmol. 2021 Nov;31(6):2818-2827. doi: 10.1177/11206721211009447. Epub 2021 Apr 23. Eur J Ophthalmol. 2021. PMID: 33892603 Review.
Cited by
-
An Unusual Case of Giant Cell Arteritis.Cureus. 2022 Jul 1;14(7):e26483. doi: 10.7759/cureus.26483. eCollection 2022 Jul. Cureus. 2022. PMID: 35919218 Free PMC article.
-
Case report: Bilateral posterior ischemic optic neuropathy in a patient with atrial fibrillation and multifocal embolic stroke.Front Neurol. 2022 Dec 2;13:988825. doi: 10.3389/fneur.2022.988825. eCollection 2022. Front Neurol. 2022. PMID: 36530620 Free PMC article.
-
Training in and comfort with diagnosis and management of ophthalmic emergencies among emergency medicine physicians in the United States.Eye (Lond). 2020 Sep;34(9):1504-1511. doi: 10.1038/s41433-020-0889-x. Epub 2020 Apr 29. Eye (Lond). 2020. PMID: 32350451 Free PMC article.
-
Orbital magnetic resonance imaging of giant cell arteritis with ocular manifestations: a systematic review and individual participant data meta-analysis.Eur Radiol. 2023 Nov;33(11):7913-7922. doi: 10.1007/s00330-023-09770-2. Epub 2023 May 31. Eur Radiol. 2023. PMID: 37256352 Free PMC article.
-
Rare Ischemic Complications of Giant Cell Arteritis: Case Series and Literature Review.Am J Case Rep. 2022 Oct 14;23:e937565. doi: 10.12659/AJCR.937565. Am J Case Rep. 2022. PMID: 36240129 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
