

Improving treatment for patients with childhood abuse related posttraumatic stress disorder (IMPACT study): protocol for a multicenter randomized trial comparing prolonged exposure with intensified prolonged exposure and phase-based treatment
- PMID: 30541492
- PMCID: PMC6291949
- DOI: 10.1186/s12888-018-1967-5
Improving treatment for patients with childhood abuse related posttraumatic stress disorder (IMPACT study): protocol for a multicenter randomized trial comparing prolonged exposure with intensified prolonged exposure and phase-based treatment
Abstract
Background: Childhood abuse related posttraumatic stress disorder (CA-PTSD) is associated with a high burden of disease and with treatment response rates that leave room for improvement. One of the treatments for PTSD, prolonged exposure (PE), is effective but has high drop-out rates and remission rates are relatively low. An intensified form of PE (iPE) was associated with good response and low drop-out rates in PTSD and has not yet been tested in a controlled trial in CA-PTSD. Phase-based treatment (PBT), in which PE is preceded by skills training may improve overall outcomes in this population. We will assess the effectiveness and cost-effectiveness of standard PE, iPE and PBT in patients with CA-PTSD.
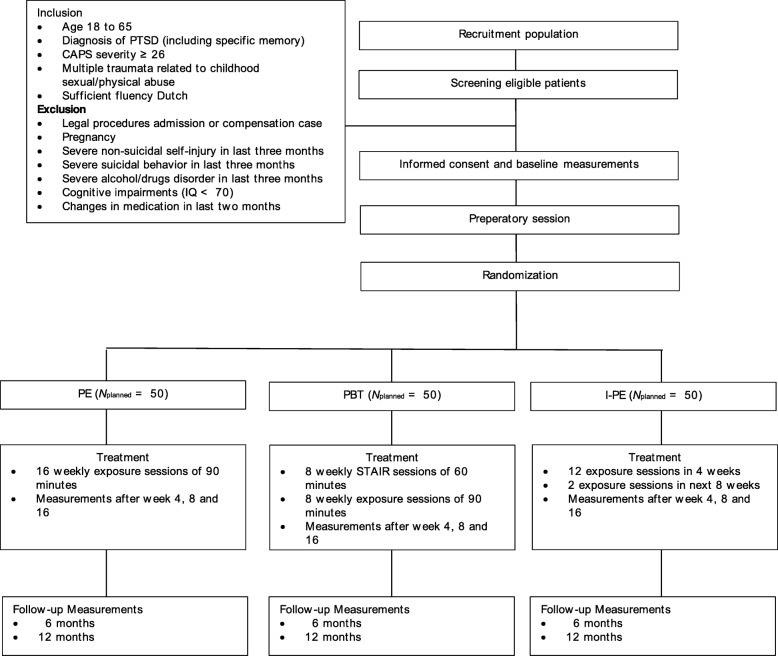
Methods/design: Multi-center randomized controlled trial. Treatment conditions are: prolonged exposure (PE; maximum of 16 sessions in 16 weeks); intensified PE (iPE; maximum of 12 sessions in four weeks and two booster sessions); phase-based treatment (PBT; maximum of eight sessions skills training followed by eight sessions PE in 16 weeks).
Primary outcome: Clinician-rated PTSD symptom severity.
Secondary outcomes: loss of PTSD diagnosis, self-reported PTSD symptom severity, comorbid symptom severity and quality of life. Moreover, we will examine cost-effectiveness and moderators and mediators of treatment outcome.
Target population: adults with CA-PTSD (N = 150). Assessments in weeks 0, 4, 8, 16, 26 and 52.
Discussion: Given that no consensus yet exists about the treatment guidelines for patients with CA-PTSD, the present study may have important implications for the treatment of CA-PTSD.
Trail registration: Registered at C.C.M.O. on Sept 7, 2016 (NL57984.058.16); retrospectively registered at June 21, 2017 at clinicaltrials.gov identifier: NCT03194113 .
Keywords: CA-PTSD; Childhood trauma; Intensive treatment; Phase-based treatment; Posttraumatic stress disorder; Prolonged exposure; STAIR; Trauma focused treatment.
Conflict of interest statement
Ethics approval and consent to participate
All participants will provide written informed consent prior to enrollment. The research protocol has been approved by the Medical Ethical Committee of Leiden University Medical Center (NL57984.058.16).
Consent for publication
Not applicable.
Competing interests
Agnes van Minnen: Receives fees from teaching and supervising clinical psychologists and psychiatrists in psychological trauma and its treatment by means of seminars, workshops and conferences, and royalties of books (Boom Publishers). Marylene Cloitre: Receives fees from teaching and consulting with mental health professionals in psychological trauma and its treatment by means of workshops, conferences and royalties from books. All other authors declare to have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Similar articles
-
Effect of Prolonged Exposure, intensified Prolonged Exposure and STAIR+Prolonged Exposure in patients with PTSD related to childhood abuse: a randomized controlled trial.Eur J Psychotraumatol. 2021 Jan 15;12(1):1851511. doi: 10.1080/20008198.2020.1851511. eCollection 2021. Eur J Psychotraumatol. 2021. PMID: 34630934 Free PMC article. Clinical Trial.
-
Phase-based treatment versus immediate trauma-focused treatment in patients with childhood trauma-related posttraumatic stress disorder: study protocol for a randomized controlled trial.Trials. 2018 Feb 22;19(1):138. doi: 10.1186/s13063-018-2508-8. Trials. 2018. PMID: 29471855 Free PMC article.
-
Skills training followed by either EMDR or narrative therapy for posttraumatic stress disorder in adult survivors of childhood abuse: a randomized controlled trial.Eur J Psychotraumatol. 2024;15(1):2332104. doi: 10.1080/20008066.2024.2332104. Epub 2024 Apr 17. Eur J Psychotraumatol. 2024. PMID: 38629403 Free PMC article. Clinical Trial.
-
Prolonged Exposure for Posttraumatic Stress Disorder in Patients Exhibiting Psychotic Symptoms: A Scoping Review.Clin Psychol Psychother. 2024 Jul-Aug;31(4):e3027. doi: 10.1002/cpp.3027. Clin Psychol Psychother. 2024. PMID: 39074495
-
An empirical review of potential mediators and mechanisms of prolonged exposure therapy.Clin Psychol Rev. 2017 Aug;56:106-121. doi: 10.1016/j.cpr.2017.07.003. Epub 2017 Jul 11. Clin Psychol Rev. 2017. PMID: 28734184 Free PMC article. Review.
Cited by
-
The effect of twice-weekly versus once-weekly sessions of either imagery rescripting or eye movement desensitization and reprocessing for adults with PTSD from childhood trauma (IREM-Freq): a study protocol for an international randomized clinical trial.Trials. 2021 Nov 27;22(1):848. doi: 10.1186/s13063-021-05712-9. Trials. 2021. PMID: 34838102 Free PMC article.
-
Impact of three variants of prolonged exposure therapy on comorbid diagnoses in patients with childhood abuse-related PTSD.Cogn Behav Ther. 2024 Jul;53(4):377-393. doi: 10.1080/16506073.2024.2318729. Epub 2024 Feb 27. Cogn Behav Ther. 2024. PMID: 38411129 Free PMC article. Clinical Trial.
-
Effect of Prolonged Exposure, intensified Prolonged Exposure and STAIR+Prolonged Exposure in patients with PTSD related to childhood abuse: a randomized controlled trial.Eur J Psychotraumatol. 2021 Jan 15;12(1):1851511. doi: 10.1080/20008198.2020.1851511. eCollection 2021. Eur J Psychotraumatol. 2021. PMID: 34630934 Free PMC article. Clinical Trial.
-
Do emotion regulation difficulties affect outcome of intensive trauma-focused treatment of patients with severe PTSD?Eur J Psychotraumatol. 2020 Feb 24;11(1):1724417. doi: 10.1080/20008198.2020.1724417. eCollection 2020. Eur J Psychotraumatol. 2020. PMID: 32166007 Free PMC article.
-
Exposure-based treatments for childhood abuse-related post-traumatic stress disorder in adults: a health-economic evaluation.Eur J Psychotraumatol. 2023;14(1):2171752. doi: 10.1080/20008066.2023.2171752. Eur J Psychotraumatol. 2023. PMID: 37052103 Free PMC article. Clinical Trial.
References
-
- Gilsanz P, Winning A, Koenen KC, Roberts AL, Sumner JA, Chen Q, Glymour MM, Rimm EB, Kubzansky LD. Post-traumatic stress disorder symptom duration and remission in relation to cardiovascular disease risk among a large cohort of women. Psychol Med. 2017;47(8):1370–1378. doi: 10.1017/S0033291716003378. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
