

In house virtual surgery and 3D complex head and neck reconstruction
- PMID: 30541624
- PMCID: PMC6290522
- DOI: 10.1186/s40463-018-0320-9
In house virtual surgery and 3D complex head and neck reconstruction
Abstract
Background: 3-Dimensional (3D) printing can be applied to virtual planning and creation of surgical guides for mandibular reconstruction. Such systems are becoming increasingly prevalent in head and neck reconstruction. However, third party access to this technology is costly and removes the opportunity to design, create, and modify the bony reconstructions, as third party technology is a black box. This series is a pilot study to document the feasibility of an in-house software tool. The objectives of this study are to describe the design of an automated in house system and assess the accuracy of this in house automated software tool for mandibular reconstruction in a simulated environment.
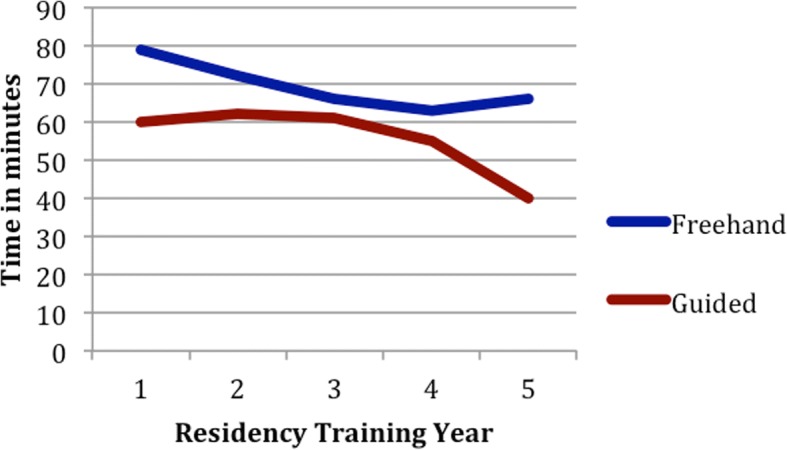
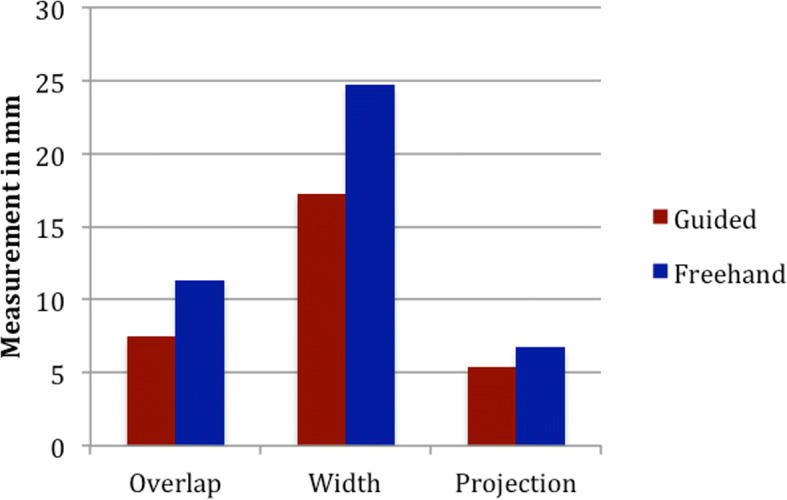
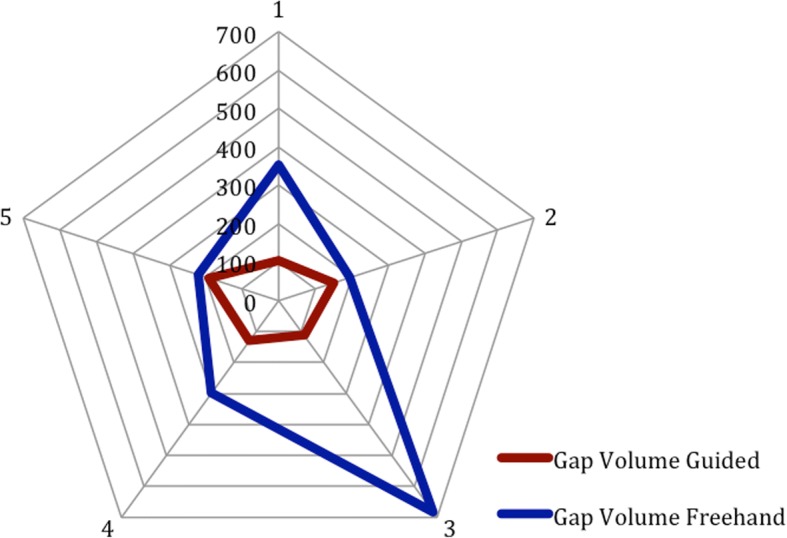
Methods: Software was written to automate the preoperative planning and surgical guide creation process. In a simulation lab, Otolaryngology residents were tasked with resecting and reconstructing a simulated mandible using the 3D-printed cutting guides. A control group of residents performed resection and reconstruction using the traditional method without cutting guides. T-test analysis was performed to compare specific aspects of the final reconstructions including: change from native mandibular width and projection, segment gap distance, and reconstruction time.
Results: Mandibular reconstruction was successful in all participants using the 3D printed system. The guided group performed significantly better on the measurement of change in Mandibular overlap, projection, segment gap volume. There was a non-significant trend towards better mandibular width and operative time for the guided group.
Conclusions: This study confirms functionality and feasibility of using an in house automated software for planning and creating surgical guides.
Keywords: 3D printing; Mandibular reconstruction; Stereolithography; Surgical cutting guide.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was obtained from the Ethics Board at the University of British Columbia. All participants read and signed a consent form prior to participation.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



Similar articles
-
New approach for virtual surgical planning and mandibular reconstruction using a fibula free flap.Oral Oncol. 2016 Aug;59:e6-e9. doi: 10.1016/j.oraloncology.2016.06.001. Epub 2016 Jun 22. Oral Oncol. 2016. PMID: 27344375
-
3D-assisted surgery for reconstruction in the head and neck area.Ugeskr Laeger. 2024 Sep 2;186(36):V04240267. doi: 10.61409/V04240267. Ugeskr Laeger. 2024. PMID: 39320075 Review. Danish.
-
Mandibular reconstruction after cancer: an in-house approach to manufacturing cutting guides.Int J Oral Maxillofac Surg. 2017 Jan;46(1):24-31. doi: 10.1016/j.ijom.2016.10.004. Epub 2016 Nov 2. Int J Oral Maxillofac Surg. 2017. PMID: 27815013
-
Accuracy and outcomes of virtual surgical planning and 3D-printed guides for osseous free flap reconstruction of mandibular osteoradionecrosis.Oral Oncol. 2022 Dec;135:106239. doi: 10.1016/j.oraloncology.2022.106239. Epub 2022 Nov 13. Oral Oncol. 2022. PMID: 36384079
-
The role of computer aided design/computer assisted manufacturing (CAD/CAM) and 3- dimensional printing in head and neck oncologic surgery: A review and future directions.Oral Oncol. 2022 Sep;132:105976. doi: 10.1016/j.oraloncology.2022.105976. Epub 2022 Jul 6. Oral Oncol. 2022. PMID: 35809506 Review.
Cited by
-
A multi-centre, participant-blinded, randomized, 3-year study to compare the efficacy of Virtual Surgical Planning (VSP) to Freehand Surgery (FHS) on bony union and quality of life outcomes for mandibular reconstruction with fibular and scapular free flaps: study protocol for a randomized phase II/III trial.BMC Cancer. 2025 Feb 27;25(1):358. doi: 10.1186/s12885-025-13505-5. BMC Cancer. 2025. PMID: 40016641 Free PMC article.
-
A Comparative Study on a Novel Fibula Malleolus Cap to Increase the Accuracy of Oncologic Jaw Reconstruction.Front Oncol. 2022 Jan 5;11:743389. doi: 10.3389/fonc.2021.743389. eCollection 2021. Front Oncol. 2022. PMID: 35070962 Free PMC article.
-
Full-Digital Workflow for Fabricating a Custom-Made Direct Metal Laser Sintering (DMLS) Mandibular Implant: A Case Report.Int J Environ Res Public Health. 2020 Apr 14;17(8):2693. doi: 10.3390/ijerph17082693. Int J Environ Res Public Health. 2020. PMID: 32295196 Free PMC article.
-
Intraoperative Real-Time Image-Guided Fibular Harvest and Mandibular Reconstruction: A Feasibility Study on Cadaveric Specimens.Head Neck. 2025 Feb;47(2):640-650. doi: 10.1002/hed.27954. Epub 2024 Oct 4. Head Neck. 2025. PMID: 39367586 Free PMC article.
-
Benefits of Patient-Specific Reconstruction Plates in Mandibular Reconstruction Surgical Simulation and Resident Education.J Clin Med. 2022 Sep 9;11(18):5306. doi: 10.3390/jcm11185306. J Clin Med. 2022. PMID: 36142953 Free PMC article.
References
-
- Matlab by Mathworks. https://www.mathworks.com (2017). Accessed Dec 2015.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
