

Dynamics of Tumor and Immune Responses during Immune Checkpoint Blockade in Non-Small Cell Lung Cancer
- PMID: 30541742
- PMCID: PMC6432636
- DOI: 10.1158/0008-5472.CAN-18-1127
Dynamics of Tumor and Immune Responses during Immune Checkpoint Blockade in Non-Small Cell Lung Cancer
Abstract
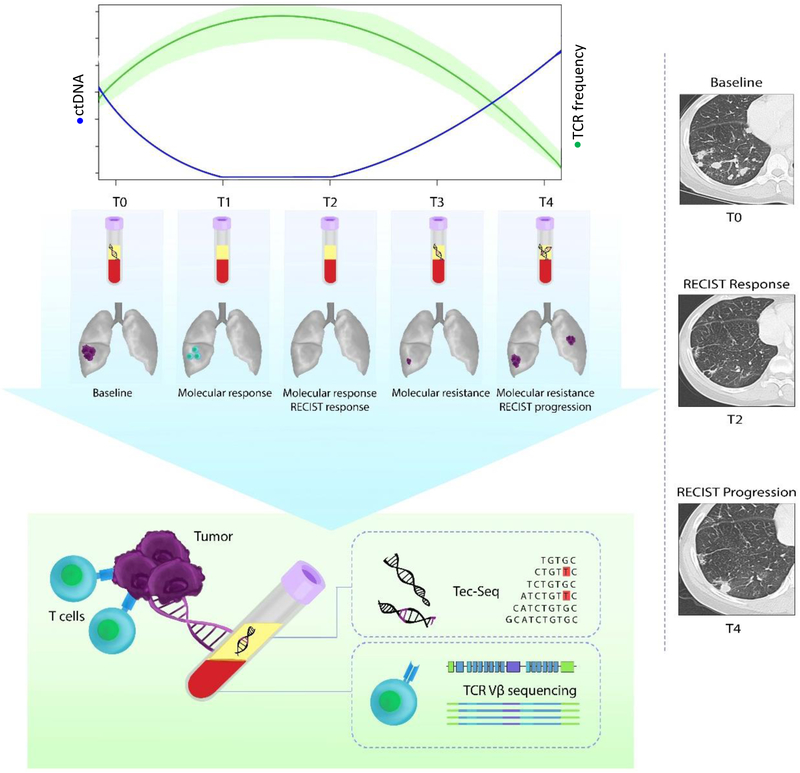
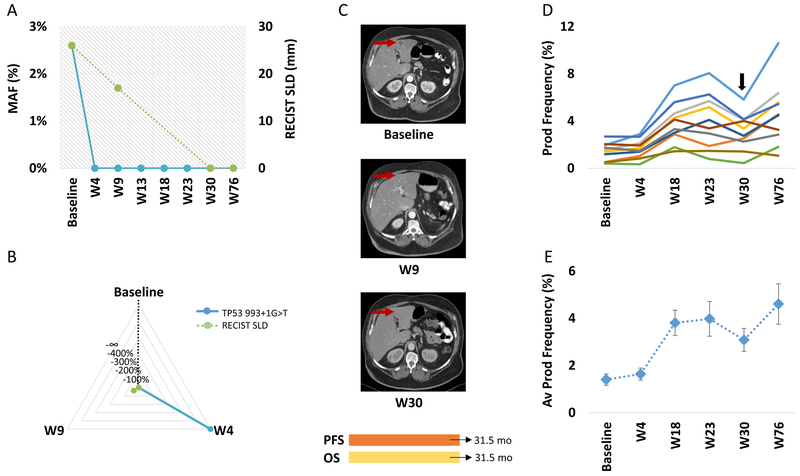
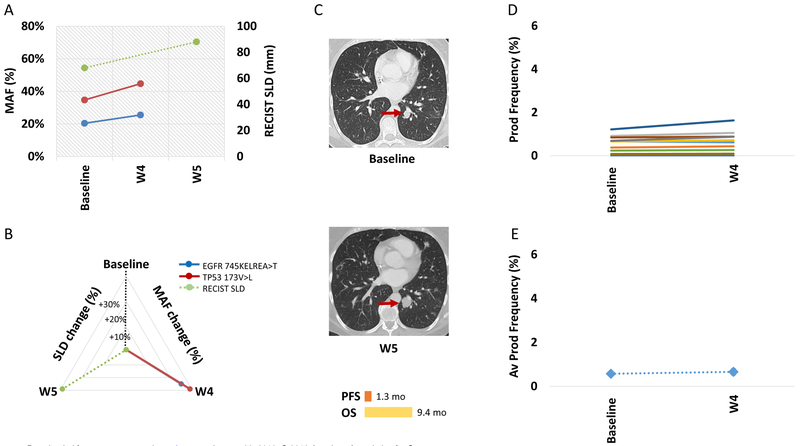
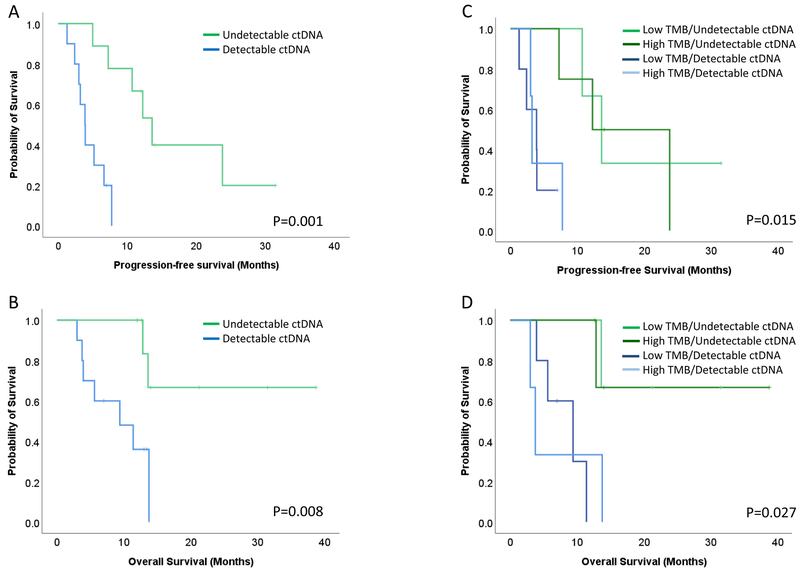
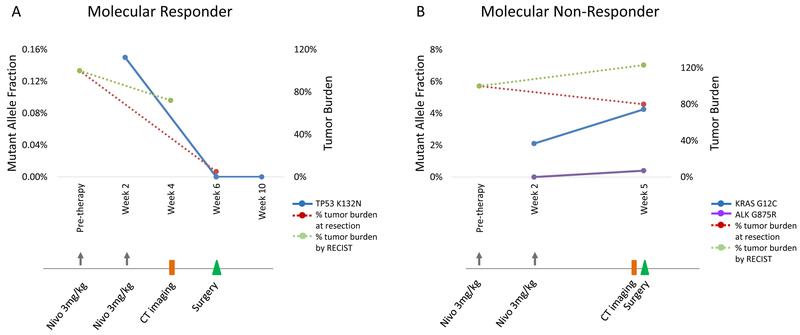
Despite the initial successes of immunotherapy, there is an urgent clinical need for molecular assays that identify patients more likely to respond. Here, we report that ultrasensitive measures of circulating tumor DNA (ctDNA) and T-cell expansion can be used to assess responses to immune checkpoint blockade in metastatic lung cancer patients (N = 24). Patients with clinical response to therapy had a complete reduction in ctDNA levels after initiation of therapy, whereas nonresponders had no significant changes or an increase in ctDNA levels. Patients with initial response followed by acquired resistance to therapy had an initial drop followed by recrudescence in ctDNA levels. Patients without a molecular response had shorter progression-free and overall survival compared with molecular responders [5.2 vs. 14.5 and 8.4 vs. 18.7 months; HR 5.36; 95% confidence interval (CI), 1.57-18.35; P = 0.007 and HR 6.91; 95% CI, 1.37-34.97; P = 0.02, respectively], which was detected on average 8.7 weeks earlier and was more predictive of clinical benefit than CT imaging. Expansion of T cells, measured through increases of T-cell receptor productive frequencies, mirrored ctDNA reduction in response to therapy. We validated this approach in an independent cohort of patients with early-stage non-small cell lung cancer (N = 14), where the therapeutic effect was measured by pathologic assessment of residual tumor after anti-PD1 therapy. Consistent with our initial findings, early ctDNA dynamics predicted pathologic response to immune checkpoint blockade. These analyses provide an approach for rapid determination of therapeutic outcomes for patients treated with immune checkpoint inhibitors and have important implications for the development of personalized immune targeted strategies.Significance: Rapid and sensitive detection of circulating tumor DNA dynamic changes and T-cell expansion can be used to guide immune targeted therapy for patients with lung cancer.See related commentary by Zou and Meyerson, p. 1038.
©2018 American Association for Cancer Research.
Figures
Comment in
-
Circulating Tumor DNA Provides a Sneak Peek into Treatment Responses in Non-Small Cell Lung Cancer.Cancer Res. 2019 Mar 15;79(6):1038-1040. doi: 10.1158/0008-5472.CAN-19-0231. Cancer Res. 2019. PMID: 30877100 Free PMC article.
References
-
- Horn L, Spigel DR, Vokes EE, Holgado E, Ready N, Steins M, et al. Nivolumab Versus Docetaxel in Previously Treated Patients With Advanced Non-Small-Cell Lung Cancer: Two-Year Outcomes From Two Randomized, Open-Label, Phase III Trials (CheckMate 017 and CheckMate 057). Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2017;35(35):3924–33. doi: 10.1200/JCO.2017.74.3062. - DOI - PMC - PubMed
-
- Anagnostou V, Yarchoan M, Hansen AR, Wang H, Verde F, Sharon E, et al. Immuno-oncology Trial Endpoints: Capturing Clinically Meaningful Activity. Clinical cancer research : an official journal of the American Association for Cancer Research. 2017;23(17):4959–69. doi: 10.1158/1078-0432.CCR-16-3065. - DOI - PMC - PubMed
-
- Bohnsack O, Hoos A, Ludajic K. Adaptation of the immune related response criteria: irRECIST. Ann Oncol. 2014;Supplement 4:iv361–iv72.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
