

Contrast-enhanced ultrasound in the diagnosis of endometrial carcinoma: A meta-analysis
- PMID: 30542488
- PMCID: PMC6257399
- DOI: 10.3892/etm.2018.6889
Contrast-enhanced ultrasound in the diagnosis of endometrial carcinoma: A meta-analysis
Abstract
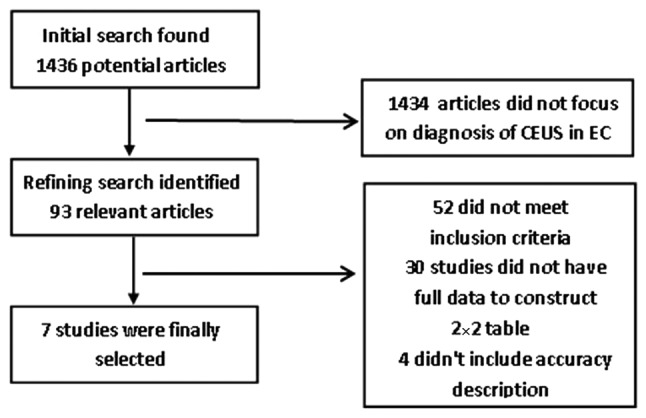
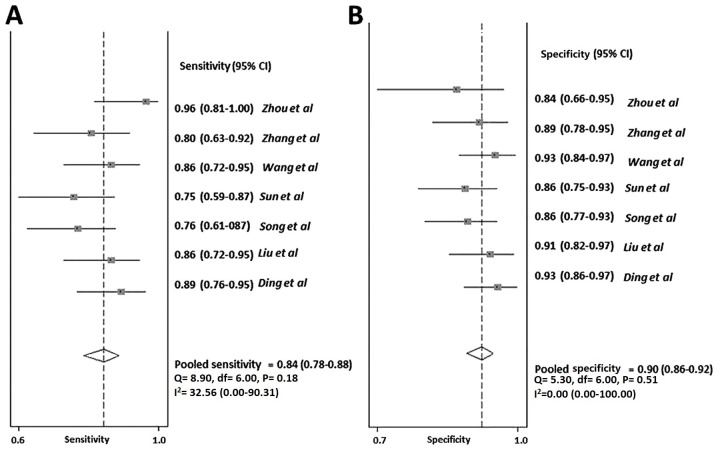
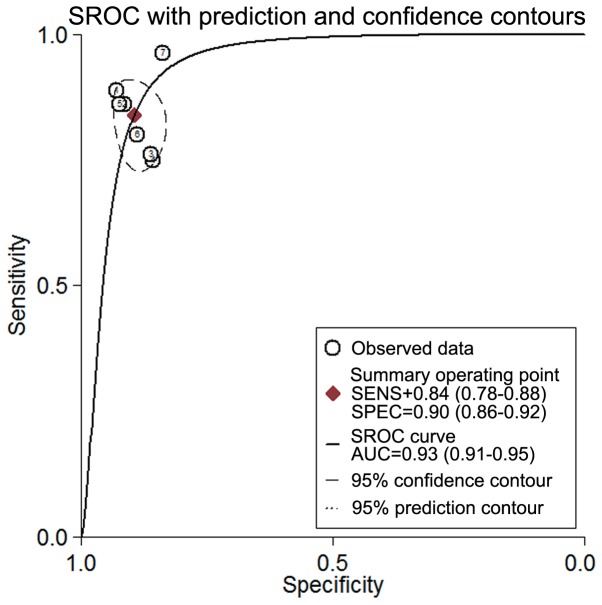
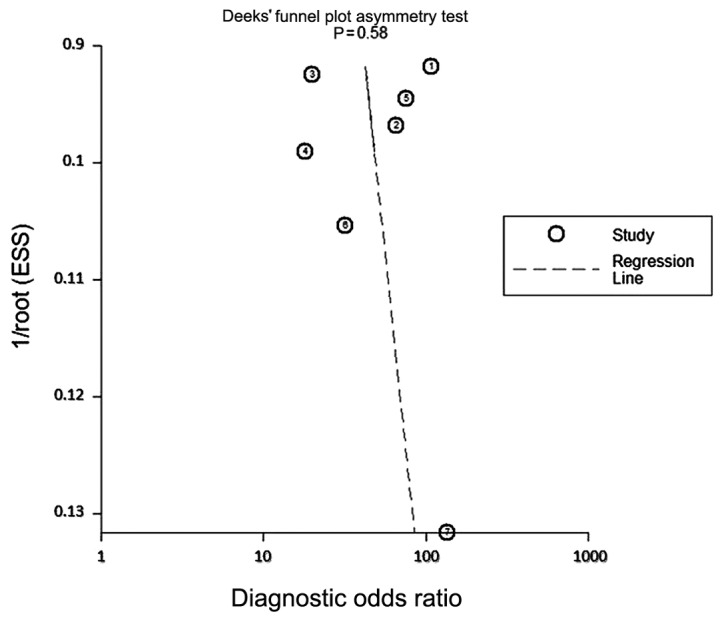
The present study evaluated the diagnostic value of contrast-enhanced ultrasound (CEUS) in endometrial carcinoma (EC). Articles published until 31 January 2017 were retrieved from PubMed, EMBASE, Elsevier, Springer and Google scholar, with the following inclusion criteria: i) The accuracy (sensitivity and specificity) of CEUS in the diagnosis of EC was evaluated; ii) a gold standard was adopted to treat and confirm EC, including surgery, histopathology and appropriate follow-up (as included in the meta-analysis); iii) the data allowed for construction of a 2×2 table of positives, false-positives, negatives and false-negatives. Pooled estimates of sensitivity, specificity, risk ratios and diagnostic odds ratios (DOR) were calculated in the present meta-analysis of the accuracy of CEUS in diagnosing EC. The summary receiver-operating characteristics (sROC) curve was also constructed. Among the 93 relevant articles, 7 studies were finally selected according to the inclusion criteria with a sample size of n=275. The pooled sensitivity of CEUS in the diagnosis of EC was 84% [95% confidence interval (CI), 0.78-0.88], while the pooled specificity was 90% (95% CI, 0.86-0.92). The positive likelihood ratio (+LR) of CEUS was 8.0 (95% CI, 5.9-10.8) and the negative likelihood ratio (-LR) was 0.18 (95% CI, 0.13-0.25). The DOR was 44 (95% CI, 26-77). The area under the sROC curve was 0.93 with specificity of 0.90 (0.86-0.92) and sensitivity of 0.84 (0.78-0.88) for the summary operating point. Moderate heterogeneity was observed for sensitivity, specificity and DOR with I2 values of 32.56, 34.68 and 41.2%, respectively. No significant publication bias was observed for the DOR of CEUS. In conclusion, the present meta-analysis indicates that CEUS is valuable in the diagnosis of EC. Additional clinical data and studies are still required to confirm these results and to further develop the diagnostic application of CEUS in EC.
Keywords: contrast-enhanced ultrasound; diagnostic accuracy; endometrial carcinoma; meta-analysis.
Figures
Similar articles
-
Diagnostic value of contrast-enhanced ultrasound for the depth of myometrial infiltration in early endometrial cancer: a meta-analysis.Front Oncol. 2025 Mar 7;15:1493246. doi: 10.3389/fonc.2025.1493246. eCollection 2025. Front Oncol. 2025. PMID: 40110205 Free PMC article.
-
Diagnostic value of contrast-enhanced ultrasound in hepatocellular carcinoma: a meta-analysis with evidence from 1998 to 2016.Oncotarget. 2017 Aug 7;8(43):75418-75426. doi: 10.18632/oncotarget.20049. eCollection 2017 Sep 26. Oncotarget. 2017. PMID: 29088877 Free PMC article.
-
Diagnostic accuracy of contrast-enhanced ultrasound for renal cell carcinoma: a meta-analysis.Tumour Biol. 2014 Jul;35(7):6343-50. doi: 10.1007/s13277-014-1815-2. Tumour Biol. 2014. PMID: 24659450
-
Diagnostic value of liver contrast-enhanced ultrasound in early hepatocellular carcinoma: a systematic review and meta-analysis.J Gastrointest Oncol. 2023 Apr 29;14(2):626-635. doi: 10.21037/jgo-23-211. Epub 2023 Apr 24. J Gastrointest Oncol. 2023. PMID: 37201077 Free PMC article.
-
Diagnostic efficacy of sentinel lymph node in breast cancer under percutaneous contrast-enhanced ultrasound: An updated meta-analysis.Thorac Cancer. 2021 Nov;12(21):2849-2856. doi: 10.1111/1759-7714.14139. Epub 2021 Oct 4. Thorac Cancer. 2021. PMID: 34605207 Free PMC article.
Cited by
-
Diagnostic value of contrast-enhanced ultrasound for the depth of myometrial infiltration in early endometrial cancer: a meta-analysis.Front Oncol. 2025 Mar 7;15:1493246. doi: 10.3389/fonc.2025.1493246. eCollection 2025. Front Oncol. 2025. PMID: 40110205 Free PMC article.
References
-
- de Boer SM, Nout RA, Jürgenliemk-Schulz IM, Jobsen JJ, Lutgens LC, van der Steen-Banasik EM, Mens JW, Slot A, Stenfert Kroese MC, Oerlemans S, et al. Long-term impact of endometrial cancer diagnosis and treatment on health-related quality of life and cancer survivorship: Results from the randomized PORTEC-2 trial. Int J Radiat Oncol Biol Phys. 2015;93:797–809. doi: 10.1016/j.ijrobp.2015.08.023. - DOI - PubMed
-
- Kurosawa H, Ito K, Nikura H, Takano T, Nagase S, Utsunomiya H, Otsuki T, Toyoshima M, Nagai T, Tanaka S, et al. Hysteroscopic inspection and total curettage are insufficient for discriminating endometrial cancer from atypical endometrial hyperplasia. Tohoku J Exp Med. 2012;228:365–70. doi: 10.1620/tjem.228.365. - DOI - PubMed
LinkOut - more resources
Full Text Sources