

Prediction of brain invasion in patients with meningiomas using preoperative magnetic resonance imaging
- PMID: 30542511
- PMCID: PMC6267603
- DOI: 10.18632/oncotarget.26313
Prediction of brain invasion in patients with meningiomas using preoperative magnetic resonance imaging
Abstract
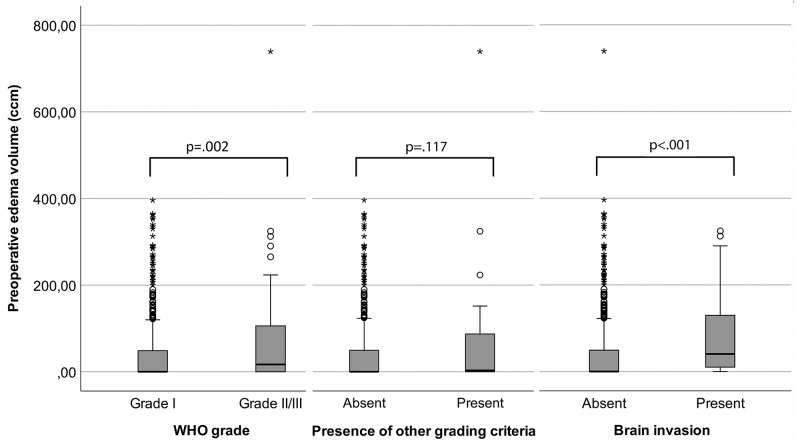
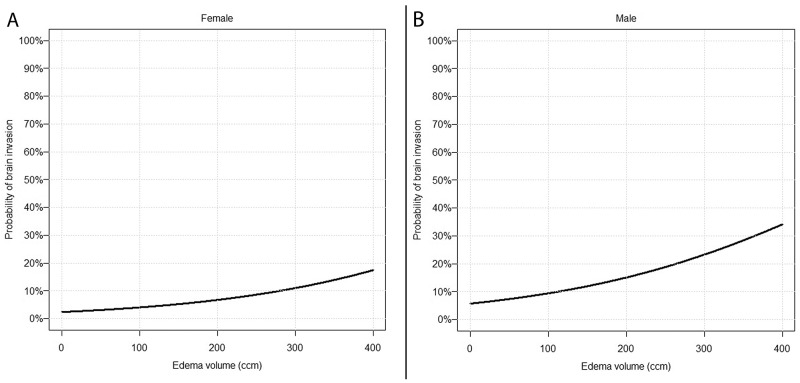
Brain invasion (BI) in meningiomas impacts WHO grading and therefore adjuvant treatment. However, BI is rare and neurosurgical sampling and neuropathological analyses are not standardised. Moreover, associations with imaging findings are sparsely known. Associations between BI and findings on preoperative MRI were investigated in 617 meningioma patients. BI was strongly correlated with other high-grade criteria (p<.001). Presence of a contrast enhancing tumour capsule, disruption of the arachnoid layer, intratumoural calcifications and T2-intensity were not related to high-grade histology or BI (p>.05, each). High-grade histology (p=.033) but not BI (p=.354) was associated with tumour location. Irregular tumour shape (OR: 3.33, 95%CI 1.33-8.30; p=.007), heterogeneous contrast enhancement (OR: 2.82, 95%CI 1.19-6.70; p=.015) and peritumoural edema (OR: 1.005 per ccm, 95%CI 1.001-1.008); p=.011) were associated with BI. Multivariable analyses identified only increasing edema volume (OR: 1.005 per ccm, 95%CI 1.002-1.009; p=.010) as a predictor for BI, independent of other histopathological high-grade criteria. We finally provide a new model to estimate the risk of BI using routine preoperative MRI. Several imaging characteristics were identified as predictors for BI. Consideration in clinical routine can increase the accuracy of the detection in neuropathological analyses.
Keywords: brain invasion; grading; magnetic resonance imaging; meningioma; radiology.
Conflict of interest statement
CONFLICTS OF INTEREST The authors report no conflict of interest concerning the material or methods used in this study or the findings specified in this paper.
Figures
References
-
- Perry A, Louis DN, von Deimling A, Sahm F, Rushing EJ, Mawrin C, Claus EB, Loeffler J, Sadetzki S. Meningiomas. In: Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Ellison DW, Figarella-Branger D, Perry A, Reifenberger G, von Deimlig A, editors. WHO Classification of Tumors of the Central Nervous System. Lyon: International Agency on Cancer Research; 2016. pp. 232–45.
-
- Heß K, Spille DC, Wagner A, Stummer W, Paulus W, Brokinkel B. Letter: brain invasion in meningiomas-sex-associated differences are not related to estrogen- and progesterone receptor expression. Neurosurgery. 2017;81:E25–27. https://doi.org/10.1093/neuros/nyx147 - DOI - PubMed
-
- Goldbrunner R, Minniti G, Preusser M, Jenkinson MD, Sallabanda K, Houdart E, von Deimling A, Stavrinou P, Lefranc F, Lund-Johansen M, Moyal EC, Brandsma D, Henriksson R, et al. EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol. 2016;17:e383–91. https://doi.org/10.1016/S1470-2045(16)30321-7 - DOI - PubMed
-
- Brokinkel B, Hess K, Mawrin C. Brain invasion in meningiomas-clinical considerations and impact of neuropathological evaluation: a systematic review. Neuro-oncol. 2017;19:1298–307. https://doi.org/10.1093/neuonc/nox071 - DOI - PMC - PubMed
-
- Jenkinson MD, Santarius T, Zadeh G, Aldape KD. Atypical meningioma-is it time to standardize surgical sampling techniques? Neuro Oncol. 2017;19:453–54. https://doi.org/10.1093/neuonc/now245 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
