

Perioperative Outcomes of Using Different Temperature Management Strategies on Pediatric Patients Undergoing Aortic Arch Surgery: A Single-Center, 8-Year Study
- PMID: 30542643
- PMCID: PMC6277883
- DOI: 10.3389/fped.2018.00356
Perioperative Outcomes of Using Different Temperature Management Strategies on Pediatric Patients Undergoing Aortic Arch Surgery: A Single-Center, 8-Year Study
Abstract
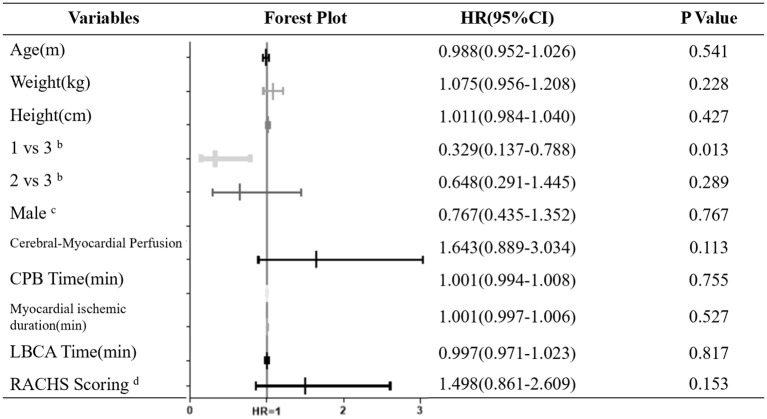
Background: With the widespread application of regional low-flow perfusion (RLFP), development of surgical techniques, and shortened circulatory arrest time, deep hypothermia is indispensable for organ protection. Clinicians have begun to increase the temperature to reduce hypothermia-related adverse outcomes. The aim of this study was to evaluate the safety and efficacy of elevated temperatures during aortic arch surgery with lower body circulatory arrest (LBCA) combined with RLFP. Methods: We retrospectively analyzed data from 207 consecutive pediatric patients who underwent aortic arch repair with LBCA & RLFP between January 2010 and July 2017 and evaluated different hypothermia management strategies. The overall cohort was divided into three groups: deep hypothermia (DH, 20.0-25.0°C), moderate hypothermia (MoH, 25.1-30.0°C) and mild hypothermia (MH, 30.1-34.0°C). Results: The percentage of AKI-1 occurrences was significantly increased in the MH group (51.52%) compared to those in the DH (25.40%) and MoH (37.84%) groups (P = 0.036); prolonged hospital stay occurrences were decreased with elevated temperature (DH 47.62%, MoH 28.83%, MH 18.18%, P = 0.006). Neurological complications, peritoneal dialysis, hepatic dysfunction, 30-day hospital mortality, delay extubation occurrences were no significant among the groups. Logistic analysis showed that the MH group was negatively associated with post-op AKI-1 compared with the DH group [OR = 0.329 (0.137-0.788), P = 0.013], no differences were found between the MoH and the MH group. Compared to other groups, the intubation time (P = 0.006) and postoperative hospital stay (P = 0.009) were significantly decreased in the MH group. Multivariate logistic analysis showed hypothermia levels were not significant with prolonged hospital stay. Conclusions: This retrospective analysis demonstrated that for pediatric patients undergoing surgeries with RLFP & LBCA, three different gradient temperature management strategies are available: deep, moderate, and mild hypothermia. Utilizing mild or moderate hypothermia is safe and feasible. Although the number of AKI-1 occurrences in the MH group was significantly increased compared to those in the other groups, further analysis showed no significance in the MoH and MH group, mild hypothermia management is as safe as others when used appropriately.
Keywords: aortic; cardiopulmonary bypass; lower body circulatory arrest; pediatric; regional low-flow perfusion.
Figures
Similar articles
-
Moderate hypothermia during aortic arch surgery is associated with reduced risk of early mortality.J Thorac Cardiovasc Surg. 2013 Sep;146(3):662-7. doi: 10.1016/j.jtcvs.2013.03.004. Epub 2013 Apr 1. J Thorac Cardiovasc Surg. 2013. PMID: 23558304
-
The safety and usefulness of cool head-warm body perfusion in aortic surgery.Eur J Cardiothorac Surg. 2000 Sep;18(3):262-9. doi: 10.1016/s1010-7940(00)00516-9. Eur J Cardiothorac Surg. 2000. PMID: 10973533
-
COMMENCE trial (Comparing hypOtherMic teMperaturEs duriNg hemiarCh surgEry): a randomized controlled trial of mild vs moderate hypothermia on patient outcomes in aortic hemiarch surgery with anterograde cerebral perfusion.Trials. 2019 Dec 9;20(1):691. doi: 10.1186/s13063-019-3713-9. Trials. 2019. PMID: 31815641 Free PMC article. Clinical Trial.
-
Is moderate hypothermic circulatory arrest with selective antegrade cerebral perfusion superior to deep hypothermic circulatory arrest in elective aortic arch surgery?Interact Cardiovasc Thorac Surg. 2016 Sep;23(3):462-8. doi: 10.1093/icvts/ivw124. Epub 2016 May 21. Interact Cardiovasc Thorac Surg. 2016. PMID: 27209532 Review.
-
Modern temperature management in aortic arch surgery: the dilemma of moderate hypothermia.Eur J Cardiothorac Surg. 2014 Jan;45(1):27-39. doi: 10.1093/ejcts/ezt154. Epub 2013 Apr 28. Eur J Cardiothorac Surg. 2014. PMID: 23628950 Review.
Cited by
-
Associations of systemic oxygen consumption with age and body temperature under general anesthesia: retrospective cohort study.BMC Anesthesiol. 2023 Jun 20;23(1):216. doi: 10.1186/s12871-023-02182-1. BMC Anesthesiol. 2023. Retraction in: BMC Anesthesiol. 2023 Oct 31;23(1):354. doi: 10.1186/s12871-023-02323-6. PMID: 37340340 Free PMC article. Retracted.
-
Association of high-sensitivity C-reactive protein and anemia with acute kidney injury in neonates.Front Pediatr. 2022 Nov 2;10:882739. doi: 10.3389/fped.2022.882739. eCollection 2022. Front Pediatr. 2022. PMID: 36405830 Free PMC article.
References
-
- Corno AF, von Segesser LK. Is hypothermia necessary in pediatric cardiac surgery? Eur J Cardiothorac Surg. (1999) 15:110–11. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous