

Projection-based respiratory-resolved left ventricular volume measurements in patients using free-breathing double golden-angle 3D radial acquisition
- PMID: 30542953
- PMCID: PMC6525134
- DOI: 10.1007/s10334-018-0727-3
Projection-based respiratory-resolved left ventricular volume measurements in patients using free-breathing double golden-angle 3D radial acquisition
Abstract
Objective: To refine a new technique to measure respiratory-resolved left ventricular end-diastolic volume (LVEDV) in mid-inspiration and mid-expiration using a respiratory self-gating technique and demonstrate clinical feasibility in patients.
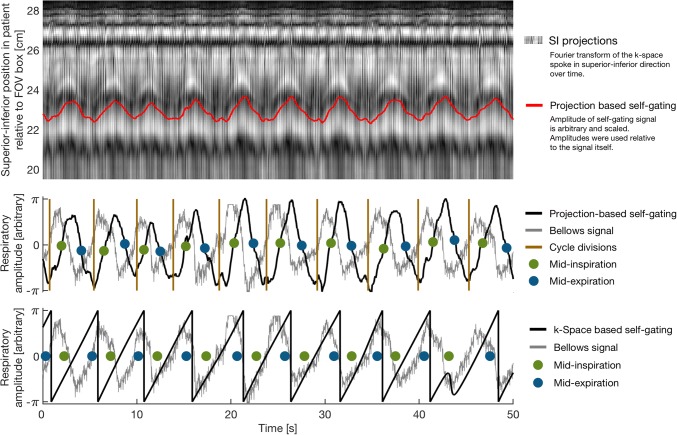
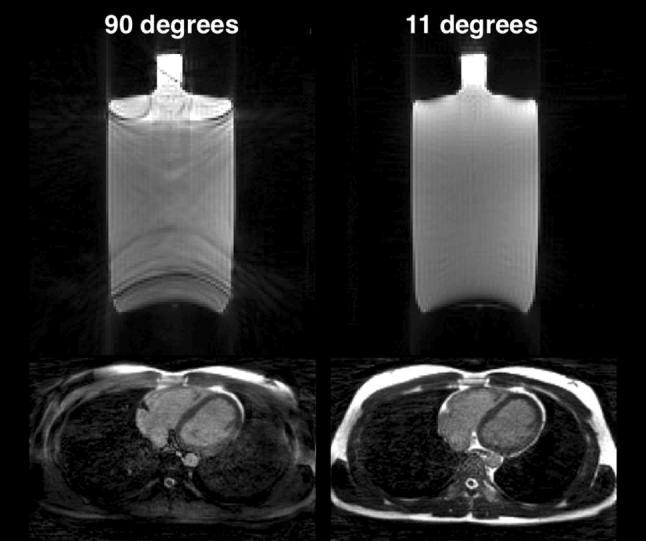
Materials and methods: Ten consecutive patients were imaged at 1.5 T during 10 min of free breathing using a 3D golden-angle radial trajectory. Two respiratory self-gating signals were extracted and compared: from the k-space center of all acquired spokes, and from a superior-inferior projection spoke repeated every 64 ms. Data were binned into end-diastole and two respiratory phases of 15% respiratory cycle duration in mid-inspiration and mid-expiration. LVED volume and septal-lateral diameter were measured from manual segmentation of the endocardial border.
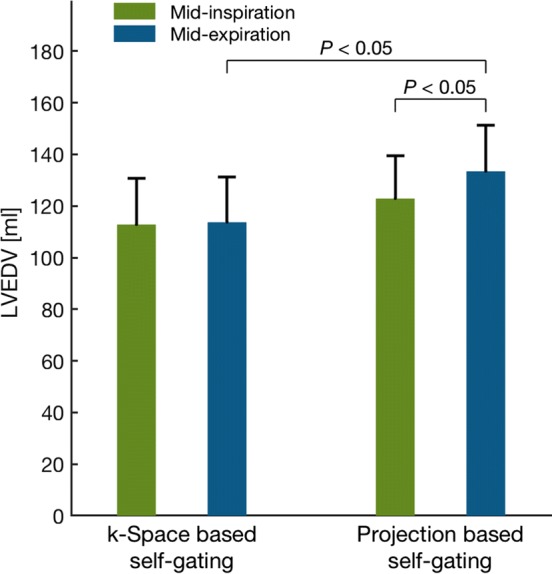
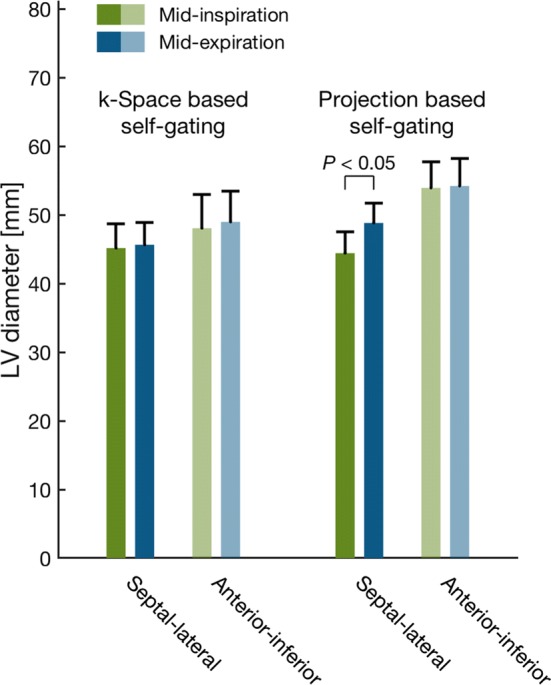
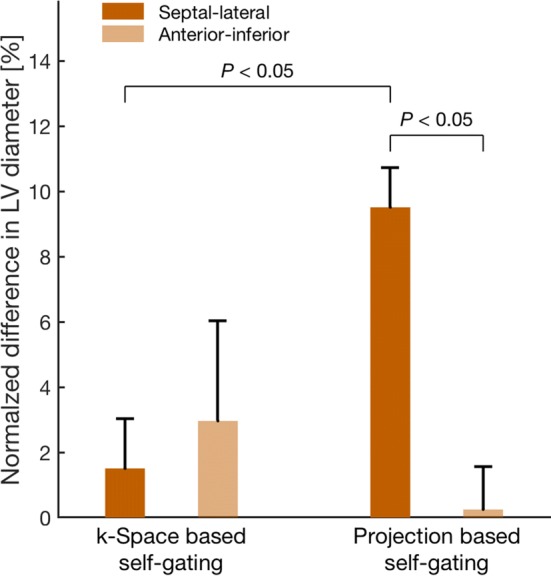
Results: Respiratory-induced variation in LVED size expressed as mid-inspiration relative to mid-expiration was, for volume, 1 ± 8% with k-space-based self-gating and 8 ± 2% with projection-based self-gating (P = 0.04), and for septal-lateral diameter, 2 ± 2% with k-space-based self-gating and 10 ± 1% with projection-based self-gating (P = 0.002).
Discussion: Measuring respiratory variation in LVED size was possible in clinical patients with projection-based respiratory self-gating, and the measured respiratory variation was consistent with previous studies on healthy volunteers. Projection-based self-gating detected a higher variation in LVED volume and diameter during respiration, compared to k-space-based self-gating.
Keywords: Cardiac imaging; Golden-angle; Radial; Respiratory resolved; Self-gating; Three-dimensional.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures




Similar articles
-
Respiratory variation in left ventricular cardiac function with 3D double golden-angle whole-heart cine imaging.Magn Reson Med. 2018 May;79(5):2693-2701. doi: 10.1002/mrm.26942. Epub 2017 Sep 17. Magn Reson Med. 2018. PMID: 28921669
-
Left ventricular volume measurements with free breathing respiratory self-gated 3-dimensional golden angle radial whole-heart cine imaging - Feasibility and reproducibility.Magn Reson Imaging. 2017 Nov;43:48-55. doi: 10.1016/j.mri.2017.07.002. Epub 2017 Jul 5. Magn Reson Imaging. 2017. PMID: 28687216
-
3D self-gated cardiac cine imaging at 3 Tesla using stack-of-stars bSSFP with tiny golden angles and compressed sensing.Magn Reson Med. 2019 May;81(5):3234-3244. doi: 10.1002/mrm.27612. Epub 2018 Nov 25. Magn Reson Med. 2019. PMID: 30474151
-
High efficiency free-breathing 3D thoracic aorta vessel wall imaging using self-gating image reconstruction.Magn Reson Imaging. 2024 Apr;107:80-87. doi: 10.1016/j.mri.2024.01.009. Epub 2024 Jan 17. Magn Reson Imaging. 2024. PMID: 38237694 Review.
-
Free-Running Cardiac and Respiratory Motion-Resolved Imaging: A Paradigm Shift for Managing Motion in Cardiac MRI?Diagnostics (Basel). 2024 Sep 3;14(17):1946. doi: 10.3390/diagnostics14171946. Diagnostics (Basel). 2024. PMID: 39272732 Free PMC article. Review.
Cited by
-
Fetal 3D cardiovascular cine image acquisition using radial sampling and compressed sensing.Magn Reson Med. 2023 Feb;89(2):594-604. doi: 10.1002/mrm.29467. Epub 2022 Sep 25. Magn Reson Med. 2023. PMID: 36156292 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
