

Efficacy and Safety of Massage for Osteoarthritis of the Knee: a Randomized Clinical Trial
- PMID: 30543021
- PMCID: PMC6420526
- DOI: 10.1007/s11606-018-4763-5
Efficacy and Safety of Massage for Osteoarthritis of the Knee: a Randomized Clinical Trial
Abstract
Background: Current treatment options for knee osteoarthritis have limited effectiveness and potentially adverse side effects. Massage may offer a safe and effective complement to the management of knee osteoarthritis.
Objective: Examine effects of whole-body massage on knee osteoarthritis, compared to active control (light-touch) and usual care.
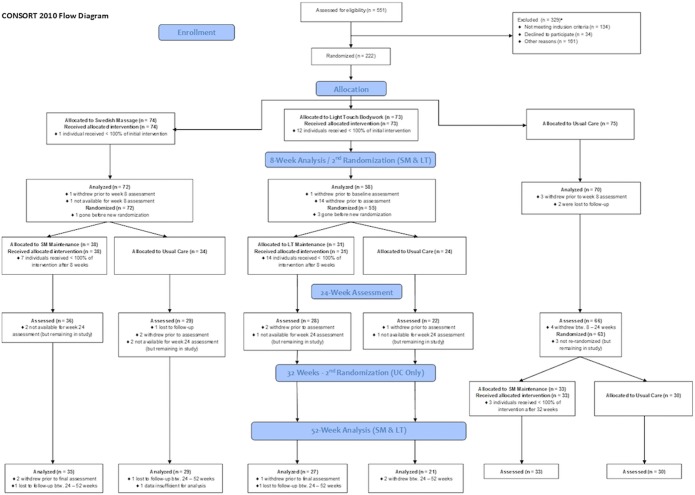
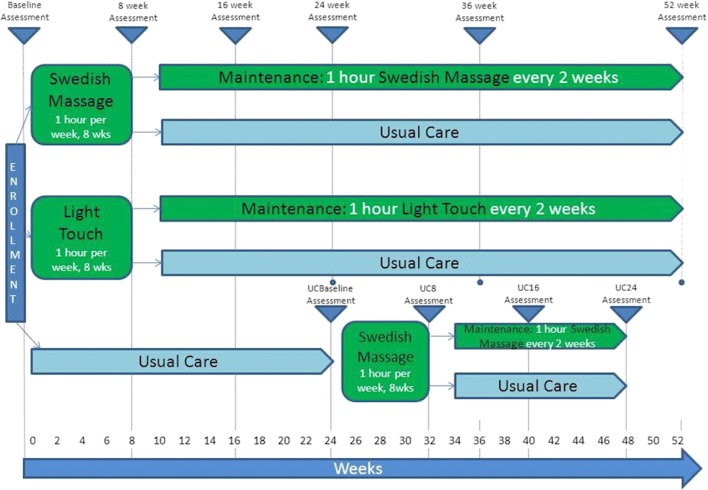
Design: Multisite RCT assessing the efficacy of massage compared to light-touch and usual care in adults with knee osteoarthritis, with assessments at baseline and weeks 8, 16, 24, 36, and 52. Subjects in massage or light-touch groups received eight weekly treatments, then were randomized to biweekly intervention or usual care to week 52. The original usual care group continued to week 24. Analysis was performed on an intention-to-treat basis.
Participants: Five hundred fifty-one screened for eligibility, 222 adults with knee osteoarthritis enrolled, 200 completed 8-week assessments, and 175 completed 52-week assessments.
Intervention: Sixty minutes of protocolized full-body massage or light-touch.
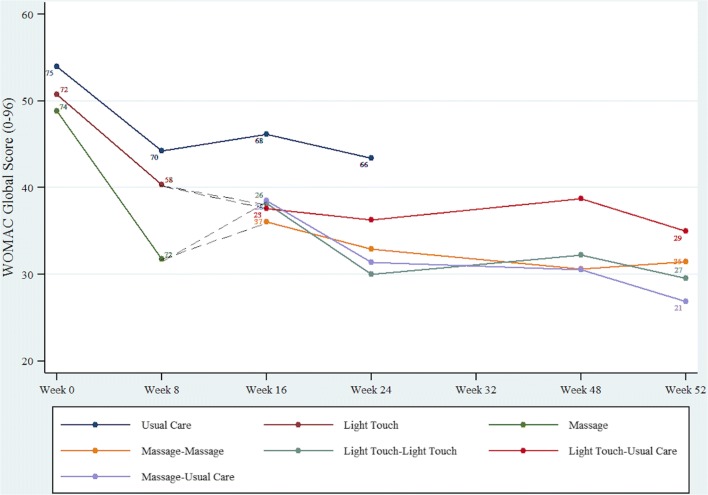
Main measures: Primary: Western Ontario and McMaster Universities Arthritis Index. Secondary: visual analog pain scale, PROMIS Pain Interference, knee range of motion, and timed 50-ft walk.
Key results: At 8 weeks, massage significantly improved WOMAC Global scores compared to light-touch (- 8.16, 95% CI = - 13.50 to - 2.81) and usual care (- 9.55, 95% CI = - 14.66 to - 4.45). Additionally, massage improved pain, stiffness, and physical function WOMAC subscale scores compared to light-touch (p < 0.001; p = 0.04; p = 0.02, respectively) and usual care (p < 0.001; p = 0.002; p = 0.002; respectively). At 52 weeks, the omnibus test of any group difference in the change in WOMAC Global from baseline to 52 weeks was not significant (p = 0.707, df = 3), indicating no significant difference in change across groups. Adverse events were minimal.
Conclusions: Efficacy of symptom relief and safety of weekly massage make it an attractive short-term treatment option for knee osteoarthritis. Longer-term biweekly dose maintained improvement, but did not provide additional benefit beyond usual care post 8-week treatment.
Trial registration: clinicaltrials.gov NCT01537484.
Keywords: arthritis; knee pain; massage; musculoskeletal pain; osteoarthritis.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
Comment in
-
Capsule Commentary on Perlman et al., Efficacy and Safety of Massage for Osteoarthritis of the Knee: a Randomized Clinical Trial.J Gen Intern Med. 2019 Mar;34(3):444. doi: 10.1007/s11606-018-4803-1. J Gen Intern Med. 2019. PMID: 30610575 Free PMC article. No abstract available.
References
-
- Arden N, Nevitt M. Osteoarthritis:epidemiology. Best Pract Res Clin Rheumatol. 2006;20:3–25. - PubMed
-
- Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation - United States, 2010-2012. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; November 8, 2013.
-
- Kato T, Xiang Y, Nakamura H, Nishioka K. Neoantigens in osteoarthritic cartilage. Curr Opin Rheumatol. 2004;16:604–608. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
