

The Temporal Relationship of Mental Health Problems and Functional Limitations following mTBI: A TRACK-TBI and TED Study
- PMID: 30543138
- PMCID: PMC6551992
- DOI: 10.1089/neu.2018.6172
The Temporal Relationship of Mental Health Problems and Functional Limitations following mTBI: A TRACK-TBI and TED Study
Abstract
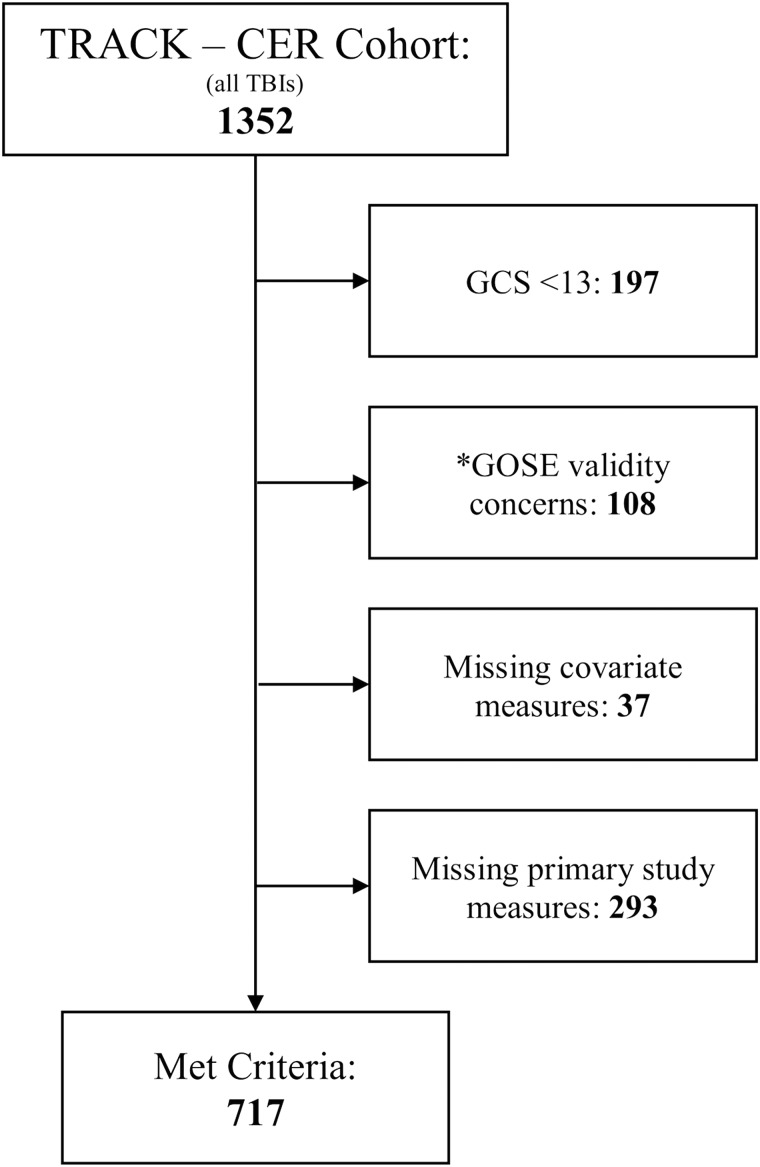
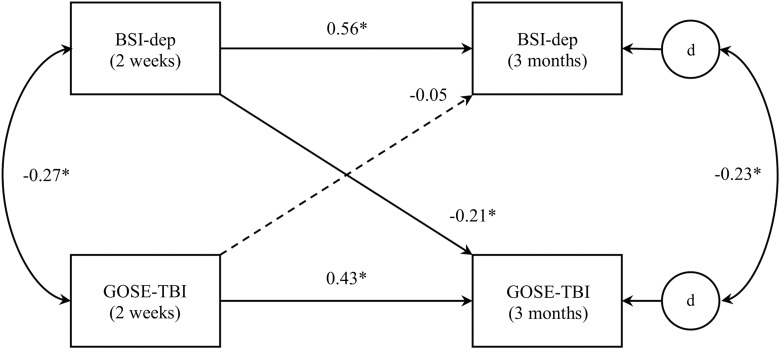
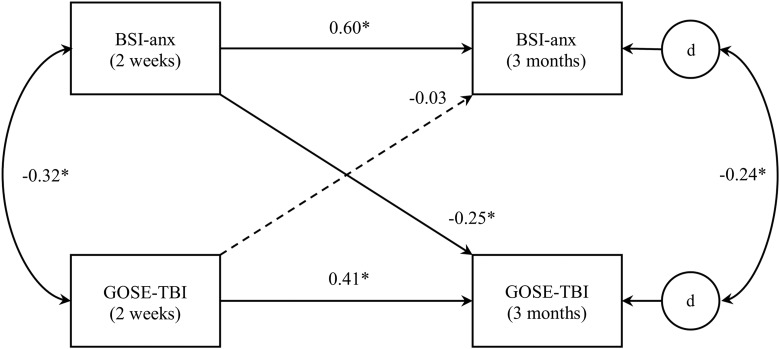
Mental health problems, such as depression and anxiety, are often associated with functional limitations after traumatic brain injury (TBI), prompting researchers to explore which of these TBI-related sequelae tends to precede the other. Past studies among patients with injuries ranging in severity have predominantly reported that functional impairments predict subsequent psychological concerns, rather than the other way around; however, it remains unclear whether this directionality holds for individuals with mild TBI (mTBI). The present study utilized a cross-lagged panel design within a structural equation modeling analytical framework to explore the longitudinal relationships of symptoms of depression and anxiety to functional status among 717 adult mTBI patients, with assessments occurring at 2 weeks and 3 months post-injury. Symptoms of both depression and anxiety significantly predicted subsequent functional limitations (λs = -0.21 and -0.25), whereas the reverse effects were nonsignificant (λs = -0.05 and -0.03); thus, psychological concerns appeared to function as a precursor to functional impairment. This pattern was particularly pronounced among patients with normal head computed tomography (CT) results; however, results were less clear cut among those subjects whose injuries were accompanied by intracranial abnormalities detected on CT imaging, suggesting the possibility of a more reciprocal relationship in the case of CT-positive mTBI. These results may serve to partially explain the incidence of persistent functional limitations observed among subsets of mTBI patients in past studies. Findings likewise highlight the importance of assessment and treatment for mental health problems after mTBI as an important factor to promote psychological well-being and functional recovery.
Keywords: brain injuries; mental health; patient outcome assessment; traumatic.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Walter W.C., and Pickett T.C. (2007). Motor impairment after severe traumatic brain injury: a longitudinal multicenter study. J. Rehabil. Res. Dev. 44, 975–982 - PubMed
-
- Dikmen S.S., Machamer J., Temkin N., and McLean A. (1990). Neuropsychological recovery in patients with moderate to severe traumatic brain injury. Arch. Phys. Med. Rehabil. 84, 1449–1475 - PubMed
-
- Hibbard M.R., Uysal S., Kepler K., Bogdany J., and Silver J. (1998). Axis I psychopathology in individuals with traumatic brain injury. J. Head Trauma Rehabil. 13, 24–39 - PubMed
-
- Deb S., Lyons I., Koutzoukis C., Ali I., and McCarthy G. (1999). Rate of psychiatric illness 1 year after traumatic brain injury. Am. J. Psychiatry 156, 374–378 - PubMed
