

Shock - Classification and Pathophysiological Principles of Therapeutics
- PMID: 30543176
- PMCID: PMC6520577
- DOI: 10.2174/1573403X15666181212125024
Shock - Classification and Pathophysiological Principles of Therapeutics
Abstract
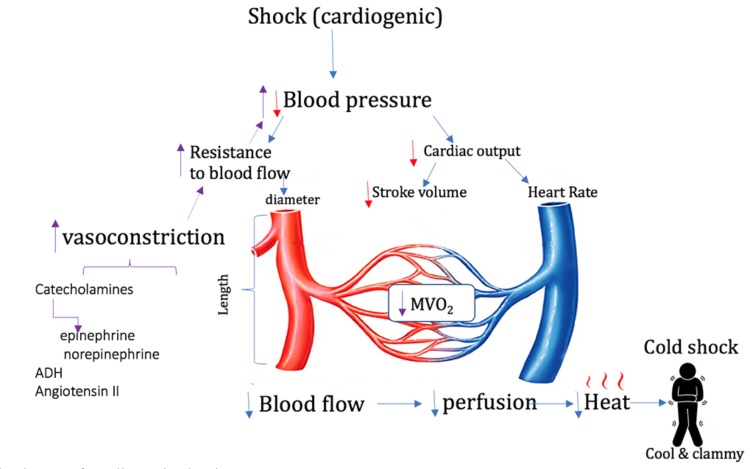
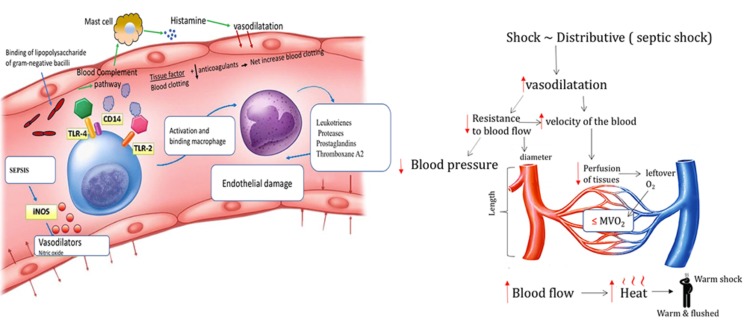
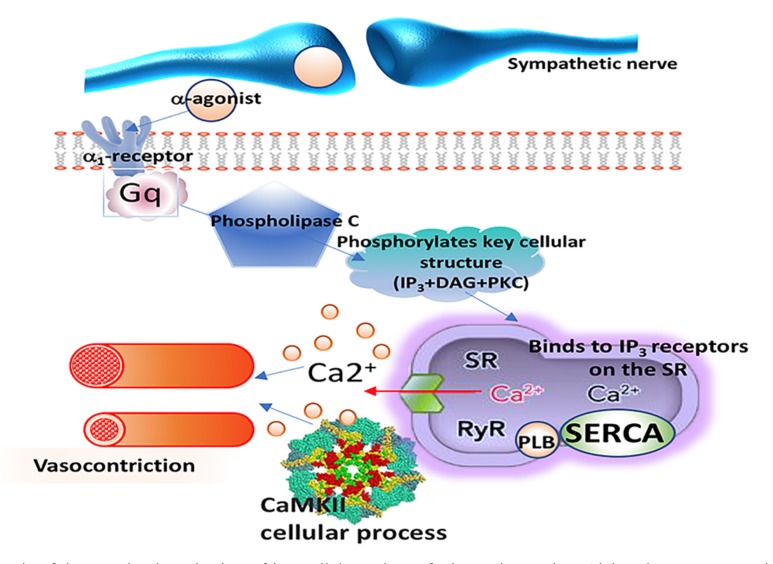
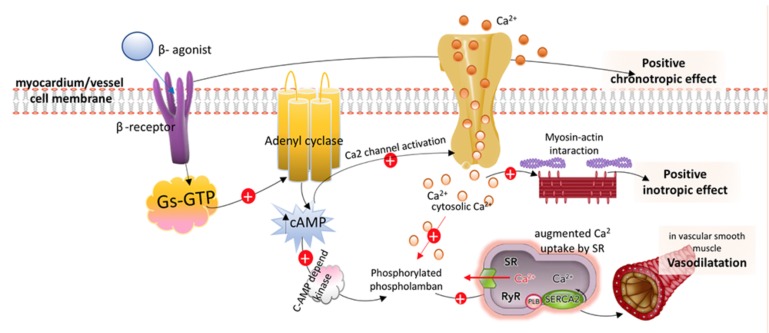
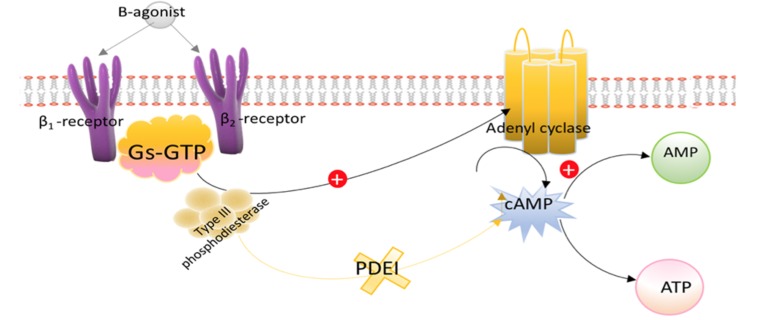
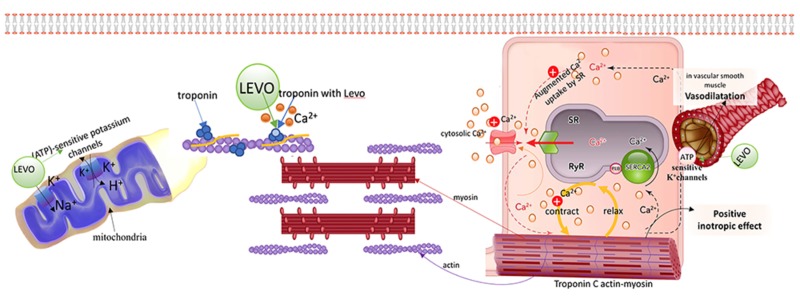
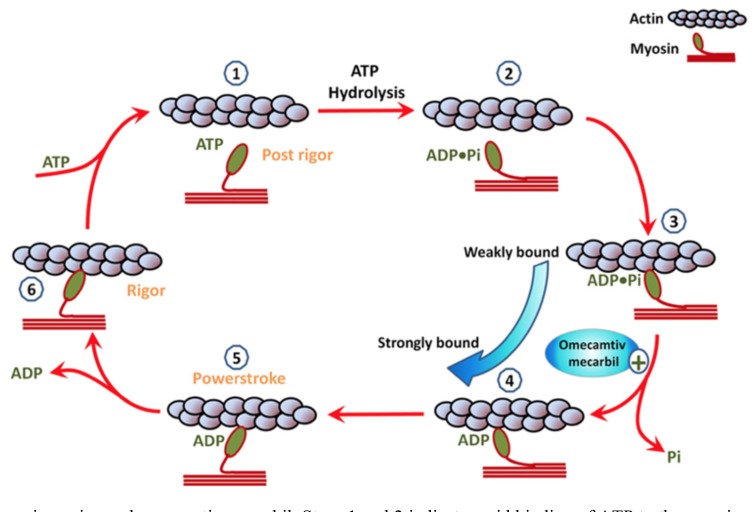
The management of patients with shock is extremely challenging because of the myriad of possible clinical presentations in cardiogenic shock, septic shock and hypovolemic shock and the limitations of contemporary therapeutic options. The treatment of shock includes the administration of endogenous catecholamines (epinephrine, norepinephrine, and dopamine) as well as various vasopressor agents that have shown efficacy in the treatment of the various types of shock. In addition to the endogenous catecholamines, dobutamine, isoproterenol, phenylephrine, and milrinone have served as the mainstays of shock therapy for several decades. Recently, experimental studies have suggested that newer agents such as vasopressin, selepressin, calcium-sensitizing agents like levosimendan, cardiac-specific myosin activators like omecamtiv mecarbil (OM), istaroxime, and natriuretic peptides like nesiritide can enhance shock therapy, especially when shock presents a more complex clinical picture than normal. However, their ability to improve clinical outcomes remains to be proven. It is the purpose of this review to describe the mechanism of action, dosage requirements, advantages and disadvantages, and specific indications and contraindications for the use of each of these catecholamines and vasopressors, as well as to elucidate the most important clinical trials that serve as the basis of contemporary shock therapy.
Keywords: Shock; cardiogenic shock; endogenous catecholamines; exogenous catecholamines; inotropes; septic shock; shock therapy; vasopressors..
Copyright© Bentham Science Publishers; For any queries, please email at epub@benthamscience.net.
Figures
References
-
- Vincent J.L., De Backer D. Circulatory shock. N. Engl. J. Med. 2013;369:1726–1734. - PubMed
-
- Russell J.A. Management of sepsis. N. Engl. J. Med. 2006;355(16):1699–1713. - PubMed
-
- Hollenberg S.M. Vasoactive drugs in circulatory shock. Am. J. Respir. Crit. Care Med. 2011;183(7):847–855. - PubMed
-
- Sato Y., Matsuzawa H., Eguchi S. Comparative study of effects of adrenaline, dobutamine and dopamine on systemic hemodynamics and renal blood flow in patients following open heart surgery. Jpn. Circ. J. 1982;46(10):1059–1072. - PubMed
-
- Butterworth JFt Dobutamine increases heart rate more than epinephrine in patients recovering from aortocoronary bypass surgery. J. Cardiothorac. Vasc. Anesth. 1992;6(5):535–541. - PubMed
