

Pulse pressure and perioperative stroke
- PMID: 30543556
- PMCID: PMC6310080
- DOI: 10.1097/ACO.0000000000000673
Pulse pressure and perioperative stroke
Abstract
Purpose of review: Central pulse pressure (PP), a marker of vascular stiffness, is a novel indicator of risk for perioperative morbidity including ischemic stroke. Appreciation for the mechanism by which vascular stiffness leads to organ dysfunction along with understanding its clinical detection may lead to improved patient management.
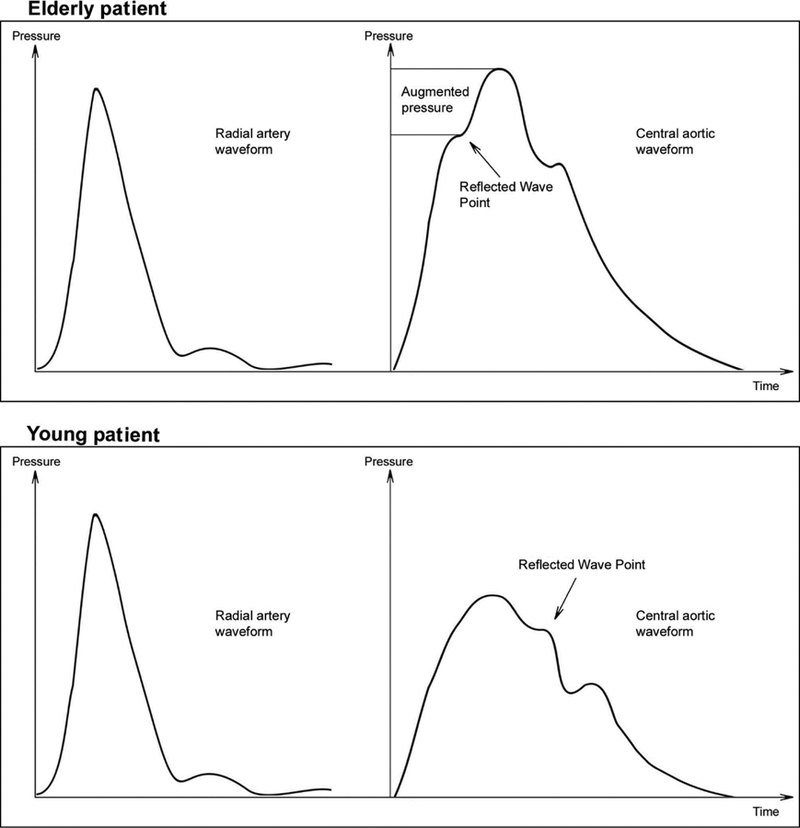
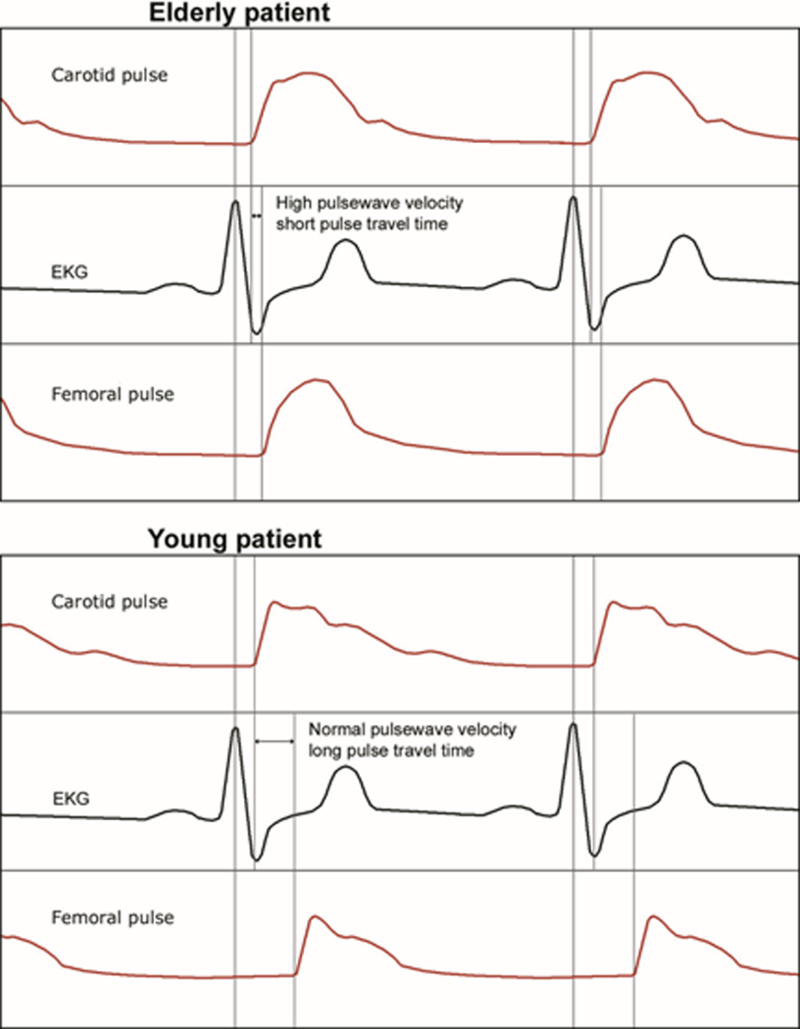
Recent findings: Vascular stiffness is associated with increased mortality and neurologic, cardiac, and renal injury in nonsurgical and surgical patients. Left ventricular hypertrophy and diastolic dysfunction along with microcirculatory changes in the low vascular resistance, high blood flow, cerebral and renal vasculature are seen in patients with vascular stiffness. Pulse wave velocity and the augmentation index have higher sensitivity for detecting of vascular stiffness than peripheral PP as the hemodynamic consequences of vascular stiffness are secondary to alterations in the central vasculature. Vascular stiffness alters cerebral autoregulation, resulting in a high likelihood of having a lower limit of autoregulation more than 65 mmHg during surgery. Vascular stiffness may predispose to cerebral hypoperfusion, increasing vulnerability to ischemic stroke, postoperative delirium, and acute kidney injury.
Summary: Vascular stiffness leads to alterations in cerebral, cardiac, and renal hemodynamics increasing the risk of perioperative ischemic stroke and neurologic, cardiac, and renal dysfunction.
Conflict of interest statement
Conflict of Interest
Dr. Hogue serves as an advisor and is paid lecturer for Medtronic, Inc (Minneapolis, MN), a maker of near infrared spectroscopy units.
Figures
Similar articles
-
Wave reflections and systemic vascular resistance are stronger determinants of pulse pressure amplification than aortic stiffness in drug-naïve hypertensives.Clin Exp Hypertens. 2020;42(3):287-293. doi: 10.1080/10641963.2019.1649684. Epub 2019 Aug 3. Clin Exp Hypertens. 2020. PMID: 31379216
-
Association Between Carotid-Cerebral Pulse Wave Velocity and Acute Ischemic Stroke: Clinical Trial Protocol.J Stroke Cerebrovasc Dis. 2019 Sep;28(9):2580-2584. doi: 10.1016/j.jstrokecerebrovasdis.2019.03.045. Epub 2019 Jun 22. J Stroke Cerebrovasc Dis. 2019. PMID: 31239221
-
Regional arterial stiffness in central and peripheral arteries is differentially related to endothelial dysfunction assessed by brachial flow-mediated dilation in metabolic syndrome.Diab Vasc Dis Res. 2018 Mar;15(2):106-113. doi: 10.1177/1479164117748840. Epub 2017 Dec 28. Diab Vasc Dis Res. 2018. PMID: 29283006
-
Arterial stiffness, pulse pressure, and the kidney.Am J Hypertens. 2015 May;28(5):561-9. doi: 10.1093/ajh/hpu206. Epub 2014 Dec 4. Am J Hypertens. 2015. PMID: 25480804 Review.
-
Arterial Flow, Pulse Pressure and Pulse Wave Velocity in Men and Women at Various Ages.Adv Exp Med Biol. 2018;1065:153-168. doi: 10.1007/978-3-319-77932-4_10. Adv Exp Med Biol. 2018. PMID: 30051383 Review.
Cited by
-
Association of Pulse Pressure Difference and Diabetes Mellitus in Chinese People: A Cohort Study.Int J Gen Med. 2021 Oct 11;14:6601-6608. doi: 10.2147/IJGM.S327841. eCollection 2021. Int J Gen Med. 2021. PMID: 34703280 Free PMC article.
-
Comparison of the efficacy and safety of remimazolam and propofol for fiberoptic bronchoscopy in older patients: a prospective, randomized controlled study.BMC Geriatr. 2025 May 14;25(1):337. doi: 10.1186/s12877-025-05984-9. BMC Geriatr. 2025. PMID: 40369438 Free PMC article. Clinical Trial.
-
Recent advances and perspectives of postoperative neurological disorders in the elderly surgical patients.CNS Neurosci Ther. 2022 Apr;28(4):470-483. doi: 10.1111/cns.13763. Epub 2021 Dec 3. CNS Neurosci Ther. 2022. PMID: 34862758 Free PMC article. Review.
-
In Vivo Quantification of Cardiac-Pulsatility-Induced Motion Before and After Double-Branched Endovascular Aortic Arch Repair.J Endovasc Ther. 2023 Aug;30(4):510-519. doi: 10.1177/15266028221086474. Epub 2022 Mar 30. J Endovasc Ther. 2023. PMID: 35352980 Free PMC article.
-
Perioperative Stroke: Mechanisms, Risk Stratification, and Management.Stroke. 2025 Sep;56(9):2798-2809. doi: 10.1161/STROKEAHA.125.051673. Epub 2025 May 30. Stroke. 2025. PMID: 40444359 Review.
References
-
- Howden L and Meyer J Age and Sex Composition: 2010. United States Census Bureau, 2011. 1–16.
-
- Aronson S, et al., Risk index for perioperative renal dysfunction/failure: critical dependence on pulse pressure hypertension. Circulation, 2007. 115: p. 733–742. - PubMed
-
- Benjo A, et al., Pulse pressure is an age-independent predictor of stroke development after cardiac surgery. Hypertension, 2007. 50: p. 630–635. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
