

Variation in severe postpartum hemorrhage management: A national vignette-based study
- PMID: 30543683
- PMCID: PMC6292622
- DOI: 10.1371/journal.pone.0209074
Variation in severe postpartum hemorrhage management: A national vignette-based study
Abstract
Objectives: To assess variations in management of severe postpartum hemorrhage: 1) between obstetricians in the same situation 2) by the same obstetrician in different situations.
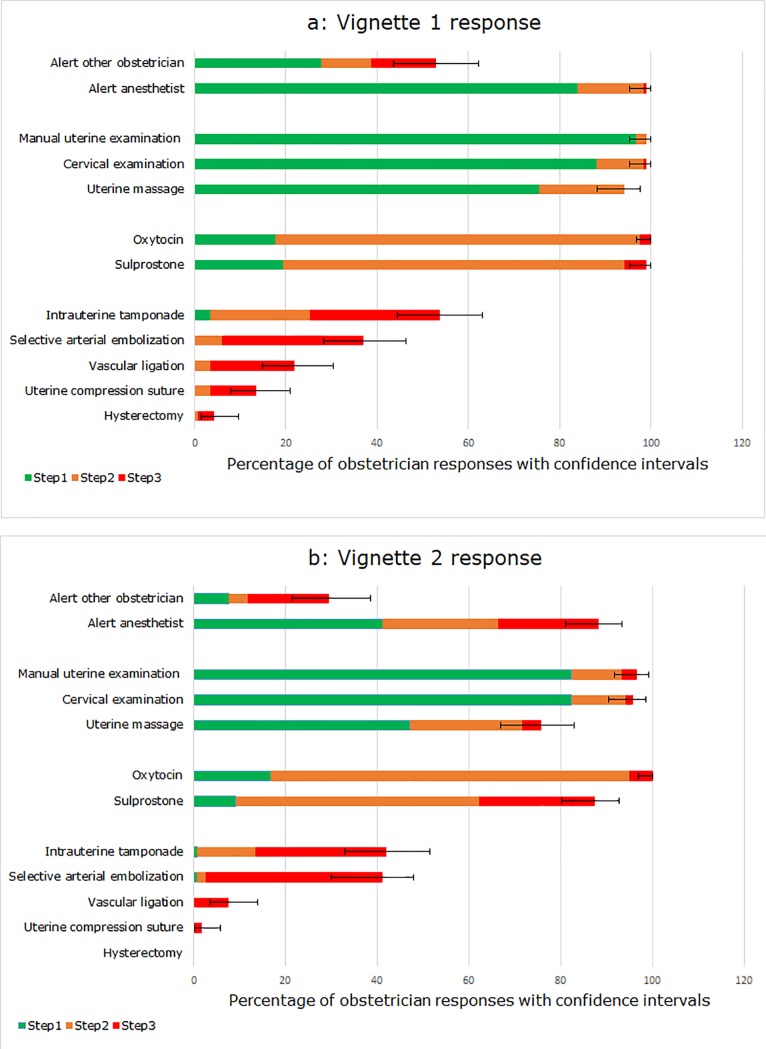
Study design: A link to a vignette-based survey was emailed to obstetricians of 215 maternity units; the questionnaire asked them to report how they would manage the PPH described in 2 previously validated case-vignettes of different scenarios of severe PPH. Vignette 1 described a typical immediate, severe PPH, and vignette 2 a less typical case of severe but gradual PPH. They were constructed in 3 successive steps and included multiple-choice questions proposing several types of clinical practice options at each step. Variations in PPH were assessed in a descriptive analysis; agreement about management and its timing between vignette 1 and vignette 2 was assessed with the Kappa coefficient.
Results: Analysis of complete responses from 119 (43.4%) obstetricians from 53 (24.6%) maternity units showed delayed or inadequate management in both vignettes. While 82.3% and 83.2% of obstetricians (in vignettes 1 and 2, respectively) would administer oxytocin 15 minutes after PPH diagnosis, only 52.9% and 29.4% would alert other team members. Management by obstetricians of the two vignette situations was inconsistent in terms of choice of treatment and timing of almost all treatments.
Conclusion: Case vignettes demonstrated inadequate management as well as variations in management between obstetricians and in different PPH situations. Protocols or procedures are necessary in all maternity units to reduce the variations in practices that may explain a part of the delay in management that leads to PPH-related maternal mortality and morbidity.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Say L, Chou D, Gemmill A, Tunçalp Ö, Moller AB, Daniels J et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014. June;2(6):e323–33. 10.1016/S2214-109X(14)70227-X - DOI - PubMed
-
- Callaghan WM, Kuklina EV, Berg CJ. Trends in postpartum hemorrhage: United States, 1994–2006. Am J Obstet Gynecol. 2010. April;202(4):353.e1–6. - PubMed
-
- Zhang W-H, Alexander S, Bouvier-Colle M-H, Macfarlane A, MOMS-B Group. Incidence of severe pre-eclampsia, postpartum haemorrhage and sepsis as a surrogate marker for severe maternal morbidity in a European population-based study: the MOMS-B survey. BJOG Int J Obstet Gynaecol. 2005. January;112(1):89–96. - PubMed
-
- Sheldon WR, Blum J, Vogel JP, Souza JP, Gülmezoglu AM, Winikoff B et al. Postpartum haemorrhage management, risks, and maternal outcomes: findings from the World Health Organization Multicountry Survey on Maternal and Newborn Health. BJOG Int J Obstet Gynaecol. 2014. March;121 Suppl 1:5–13. - PubMed
-
- Committee on Practice Bulletins-Obstetrics. Practice Bulletin No. 183: Postpartum Hemorrhage. Obstet Gynecol. 2017;130(4):e168–86. 10.1097/AOG.0000000000002351 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
