

Case Reports
doi: 10.1016/j.jtho.2018.11.031.
Epub 2018 Dec 10.
Small Cell Lung Cancer Transformation as a Mechanism of Resistance to PD-1 Therapy in KRAS-Mutant Lung Adenocarcinoma: A Report of Two Cases
Affiliations
- PMID: 30543839
- PMCID: PMC6382512
- DOI: 10.1016/j.jtho.2018.11.031
Item in Clipboard
Case Reports
Small Cell Lung Cancer Transformation as a Mechanism of Resistance to PD-1 Therapy in KRAS-Mutant Lung Adenocarcinoma: A Report of Two Cases
J Thorac Oncol.
2019 Mar.
No abstract available
Figures
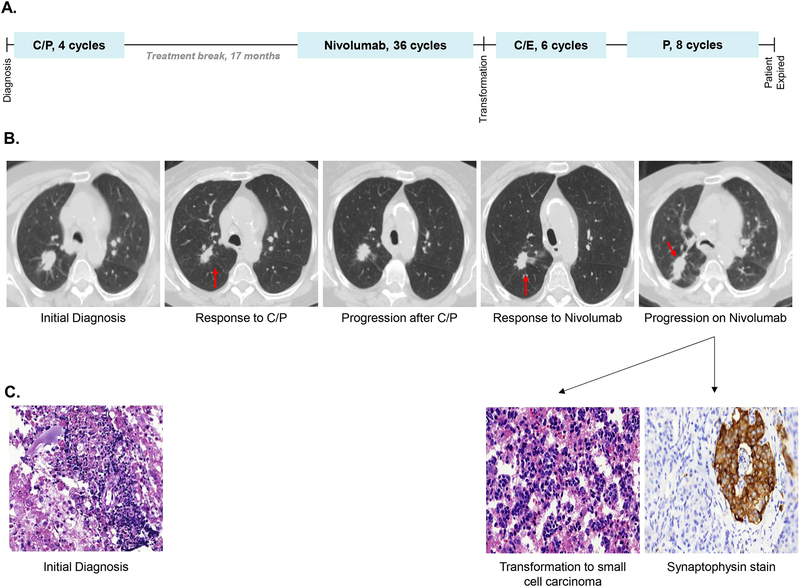
(A) The patient received four cycles of carboplatin and paclitaxel (C/P) followed by a 17 month therapy holiday. She then received 36 cycles of nivolumab every two weeks with an initial response, and two weeks after her 36th dose of nivolumab she had widespread disease progression with biopsy revealing transformation to small cell carcinoma. She went on to receive six cycles of carboplatin and etoposide (C/E) and had a partial response. Two months after completion of C/E she had disease progression and received eight cycles of paclitaxel (P) with a response in her thoracic disease, but she had progression in the central nervous system prior to her death 11 months after small cell transformation. (B) Treatment responses were observed in the primary right upper lobe nodule (red arrow) to both carboplatin and paclitaxel and nivolumab, followed by widespread progression, including in the right upper lobe nodule (red arrow), at the time of transformation to small cell carcinoma. (C) Pathology from a level 4R lymph node at the time of diagnosis demonstrated poorly differentiated adenocarcinoma. Cytology from pericardial fluid at the time of transformation demonstrated small cell carcinoma, confirmed by synaptophysin immunohistochemistry.
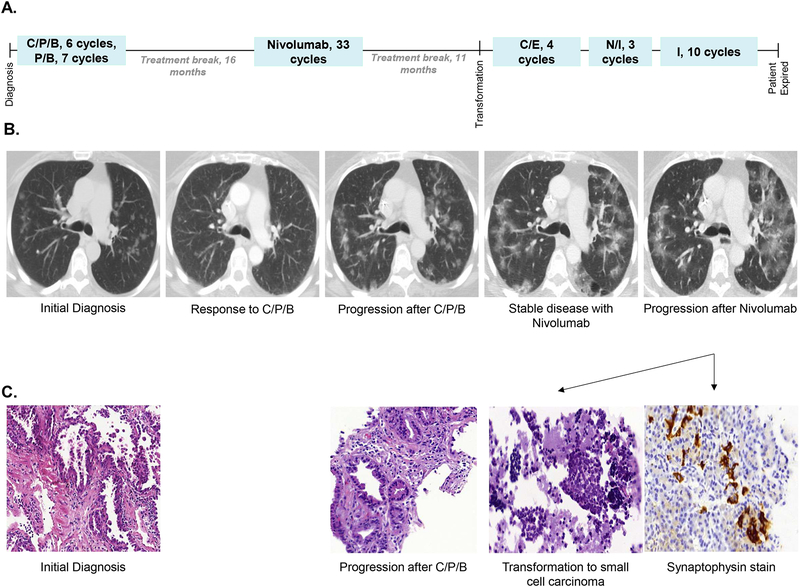
(A) The patient received six cycles of carboplatin, pemetrexed, and bevacizumab (C/P/B), followed by seven cycles of pemetrexed and bevacizumab maintenance. She experienced disease progression after a 16 month therapy holiday. She received 33 cycles of second line nivolumab with disease stabilization, and after an 11 month therapy holiday she progressed with transformation to small cell carcinoma. She received four cycles of carboplatin and etoposide (C/E) with disease stabilization, and then experienced disease progression four months after completion of C/E. She received three cycles of nivolumab and ipilimumab (N/I) with disease progression, then received 10 cycles of irinotecan (I) with initial disease stabilization. After 10 cycles of irinotecan she had further disease progression, and then transitioned to hospice care dying 16 months after small cell transformation. (B) The patient’s disease was primarily measured by upper lobe ground glass opacities (GGOs). She experienced a partial response by RECIST criteria with first line therapy, then disease stabilization on second line nivolumab. She had asymptomatic diffuse progression of her bilateral GGOs at the time of transformation to small cell carcinoma. (C) Pathology from a left lower lobe lesion at the time of diagnosis demonstrated lung adenocarcinoma. At the time of first progression pathology from a right lower lobe lesion revealed lung adenocarcinoma consistent with the prior diagnosis. Pathology from a station 7 lymph node at the time of second progression demonstrated small cell carcinoma, confirmed by synaptophysin immunohistochemistry.
References
-
- Lee JK, Lee J, Kim S, et al. Clonal History and Genetic Predictors of Transformation Into Small-Cell Carcinomas From Lung Adenocarcinomas. J Clin Oncol 2017;35:3065–74. - PubMed
-
- Sutherland KD, Proost N, Brouns I, Adriaensen D, Song JY, Berns A. Cell of origin of small cell lung cancer: inactivation of Trp53 and Rb1 in distinct cell types of adult mouse lung. Cancer Cell 2011;19:754–64. - PubMed
-
- Norkowski E, Ghigna MR, Lacroix L, et al. Small-cell carcinoma in the setting of pulmonary adenocarcinoma: new insights in the era of molecular pathology. J Thorac Oncol 2013;8:1265–71. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
