

Deterioration in right ventricular structure and function over time in patients with heart failure and preserved ejection fraction
- PMID: 30544228
- PMCID: PMC7963126
- DOI: 10.1093/eurheartj/ehy809
Deterioration in right ventricular structure and function over time in patients with heart failure and preserved ejection fraction
Abstract
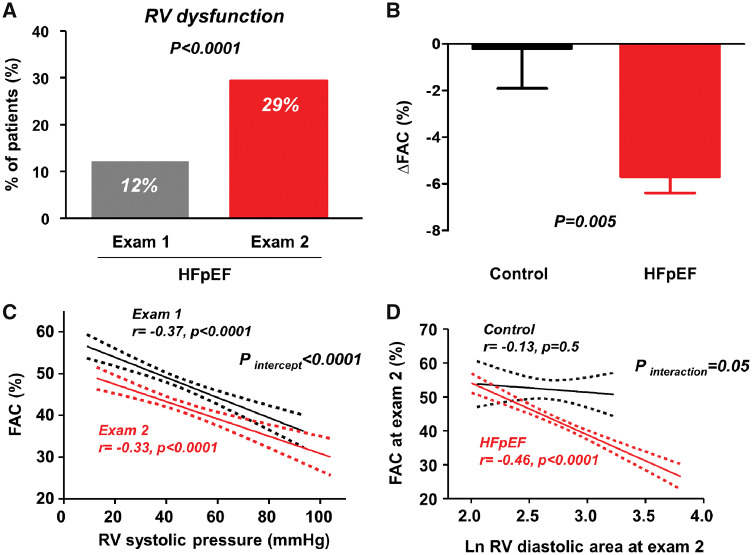
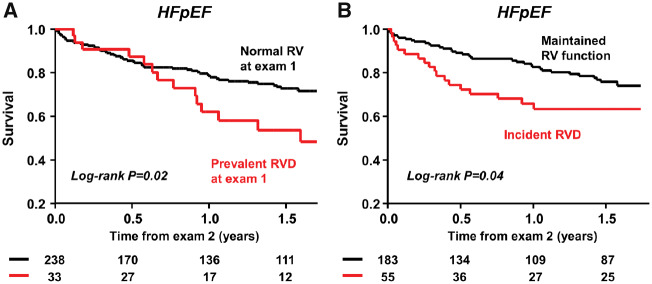
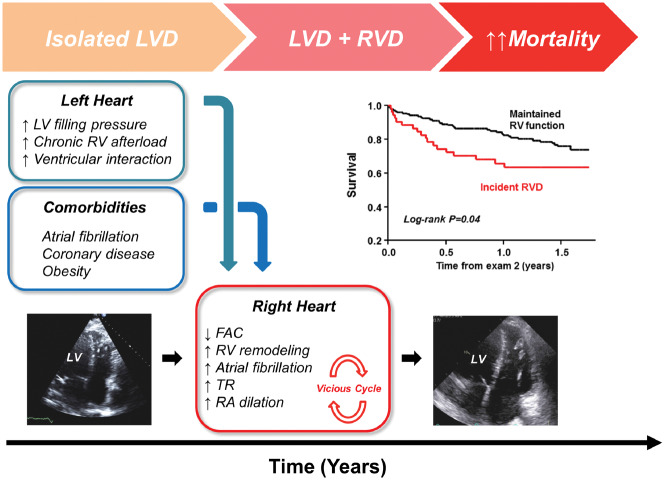
Aims: Prevalent right ventricular (RV) dysfunction (RVD) is associated with increased mortality in patients with heart failure with preserved ejection fraction (HFpEF), but no study has characterized long-term changes in RV structure and function within the same patient.
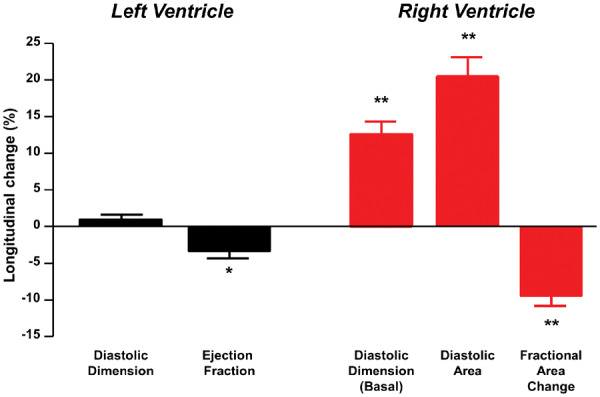
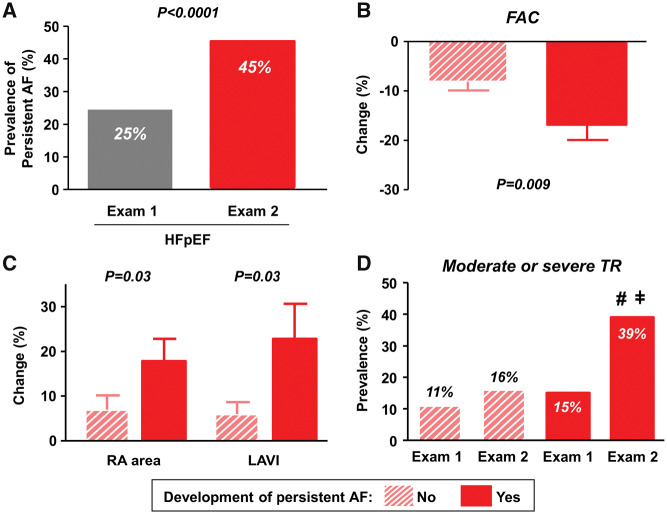
Methods and results: Patients with unequivocal HFpEF defined by either invasive haemodynamics or hospitalization for pulmonary oedema (n = 271) underwent serial echocardiographic evaluations >6 months apart. Clinical, structural, functional, and haemodynamic characteristics were examined. Over a median of 4.0 years (interquartile range 2.1-6.1), there was a 10% decline in RV fractional area change and 21% increase in RV diastolic area (both P < 0.0001). These changes greatly exceeded corresponding changes in the left ventricle. The prevalence of tricuspid regurgitation increased by 45%. Of 238 patients with normal RV function at Exam 1, 55 (23%) developed RVD during follow-up. Development of RVD was associated with both prevalent and incident atrial fibrillation (AF), higher body weight, coronary disease, higher pulmonary artery and left ventricular filling pressures, and RV dilation. Patients with HFpEF developing incident RVD had nearly two-fold increased risk of death (adjusted hazard ratio 1.89, 95% confidence interval 1.01-3.44; P = 0.04).
Conclusion: While previous attention has centred on the left ventricle in HFpEF, these data show that right ventricular structure and function deteriorate to greater extent over time when compared with changes in the left ventricle. Further study is required to evaluate whether interventions targeting modifiable risk factors identified for incident RVD, including abnormal haemodynamics, AF, coronary disease, and obesity, can prevent RVD and thus improve outcomes.
Keywords: Atrial fibrillation; HFpEF; Heart failure; Pulmonary hypertension; Right ventricle; Tricuspid regurgitation.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2018. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Rapid right-sided deterioration in heart failure with preserved ejection fraction.Eur Heart J. 2019 Feb 21;40(8):699-702. doi: 10.1093/eurheartj/ehy900. Eur Heart J. 2019. PMID: 30608519 No abstract available.
References
-
- Reddy YN, Borlaug BA. Heart failure with preserved ejection fraction. Curr Probl Cardiol 2016;41:145–188. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
