

Transition of a Mallory-Weiss syndrome to a Boerhaave syndrome confirmed by anamnestic, necroscopic, and autopsy data: A case report
- PMID: 30544378
- PMCID: PMC6310542
- DOI: 10.1097/MD.0000000000013191
Transition of a Mallory-Weiss syndrome to a Boerhaave syndrome confirmed by anamnestic, necroscopic, and autopsy data: A case report
Abstract
Rationale: Spontaneous esophageal rupture (Boerhaave syndrome) is a rare, though frequently fatal, event. It is generally caused by a sudden increase in pressure inside the esophagus. In some cases, full-thickness perforations of the esophagus may develop from previous lesions that initially involve only the esophageal mucosa (Mallory-Weiss syndrome) and which, following further triggering events, give rise to a transmural lesion.
Patient concerns: Here, we present the case of a 45-year-old subject who suddenly died of acute cardio-respiratory failure, an autopsy was performed to identify the cause of death.
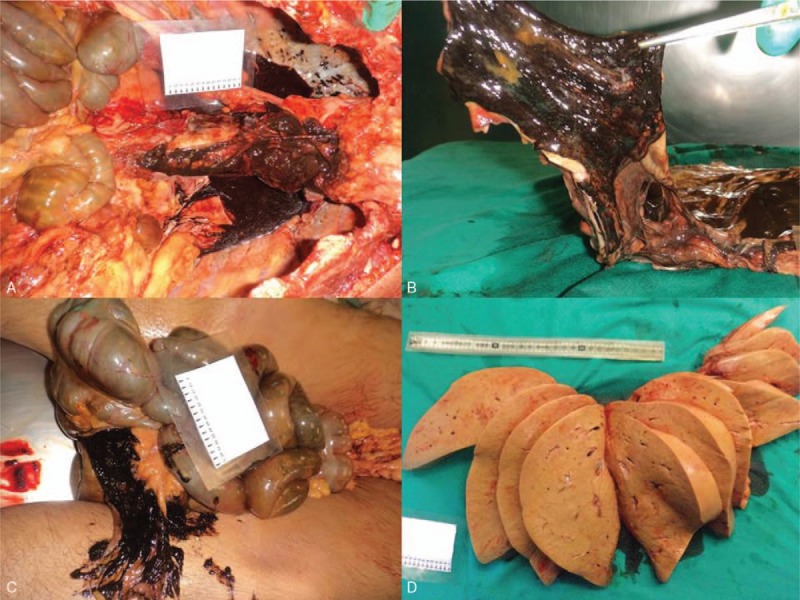
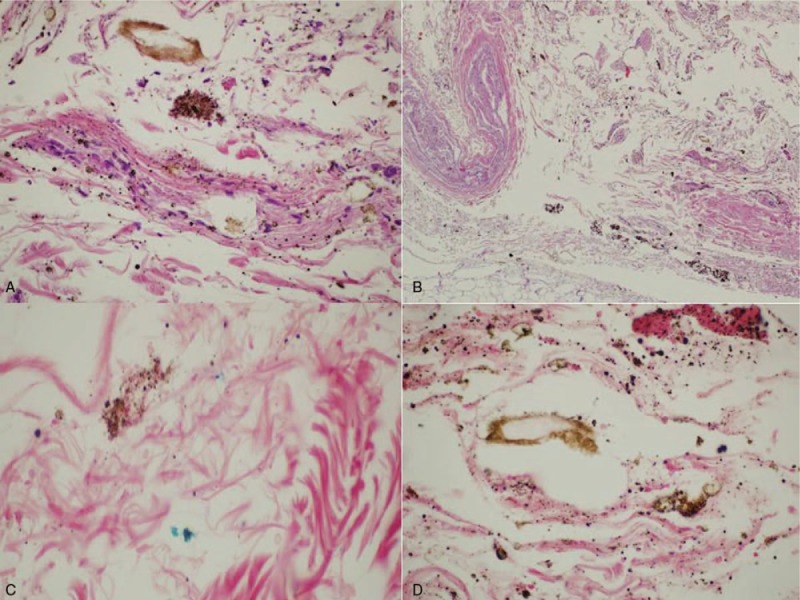
Diagnosis, interventions, and outcomes: The autopsy examination revealed a full-thickness rupture of the esophageal wall. Through the integration of necroscopy findings, anamnestic data, and histopathological examination, it has been possible to establish that complete esophageal rupture resulted from the evolution of a previous partial lesion of the esophageal wall, and that an untreated Mallory-Weiss syndrome evolved into a rapidly fatal Boerhaave syndrome.
Lessons: This case shows that distal esophageal tears, rather than constituting a distinct entity, may be part of a spectrum of diseases and that a partial lesion of the esophageal wall caused by barogenic injury may evolve into a full-thickness rupture following further barotraumas.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Chirica M, Champault A, Dray X, et al. Esophageal perforations. J Visc Surg 2010;147:e117–28. - PubMed
-
- Beal SL, Pottmeyer EW, Spisso JM. Esophageal perforation following external blunt trauma. J Trauma 1988;28:1425–32. - PubMed
-
- Grey TC, Mittleman RE, Wetli CV, et al. Aortoesophageal fistula and sudden death. A report of two cases and review of the literature. Am J Forensic Med Pathol 1988;9:19–22. - PubMed
-
- Brinster CJ, Singhal S, Lee L, et al. Evolving options in the management of esophageal perforation. Ann Thorac Surg 2004;77:1475–83. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
