

A new scoring model predicting macroscopic vascular invasion of early-intermediate hepatocellular carcinoma
- PMID: 30544459
- PMCID: PMC6310496
- DOI: 10.1097/MD.0000000000013536
A new scoring model predicting macroscopic vascular invasion of early-intermediate hepatocellular carcinoma
Abstract
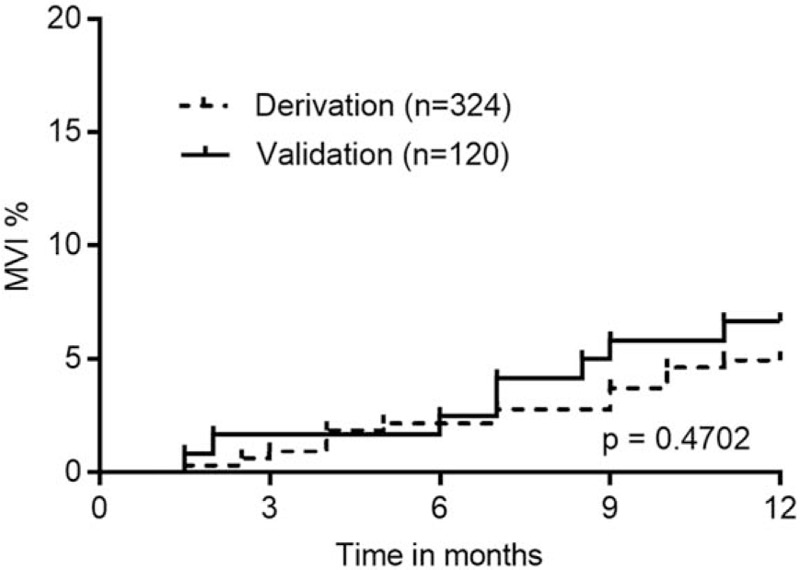
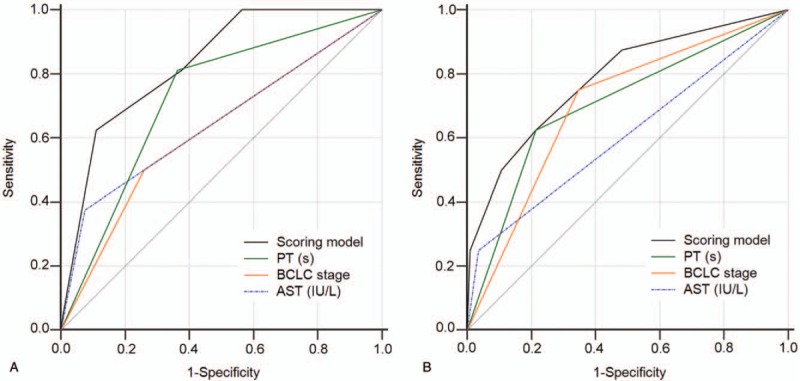
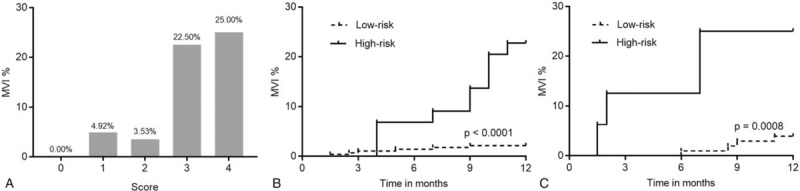
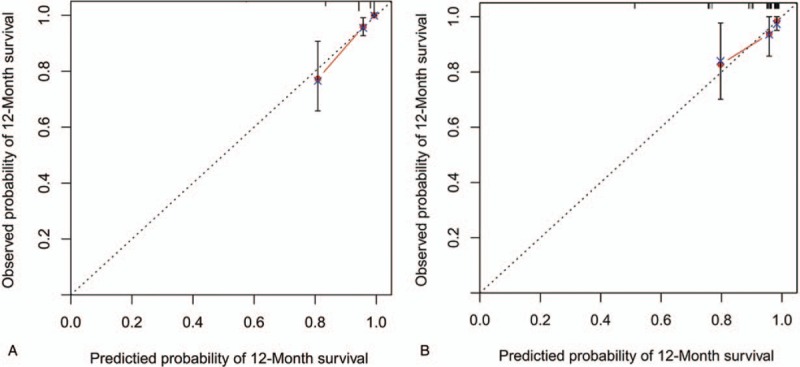
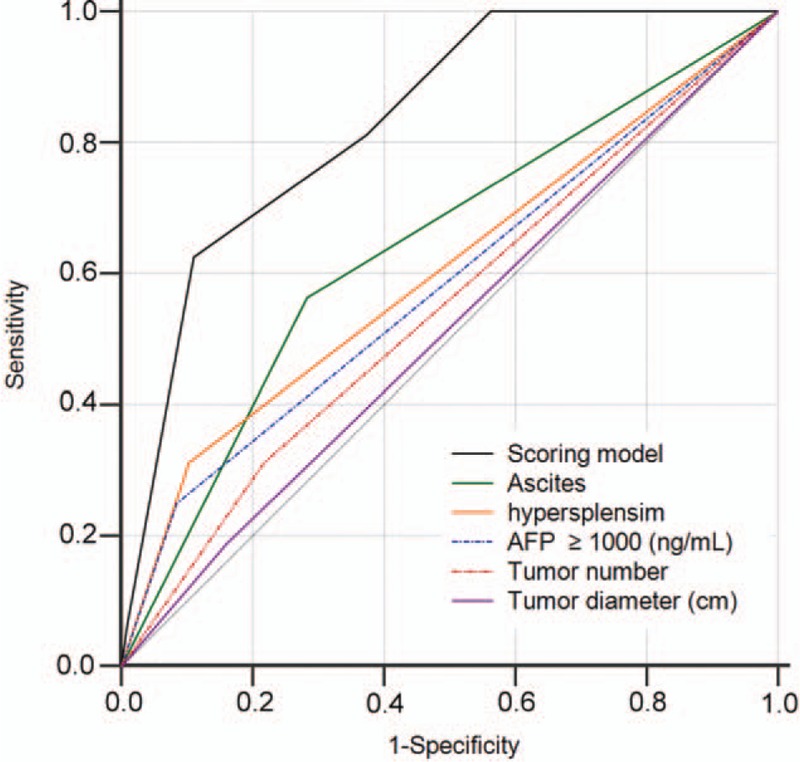
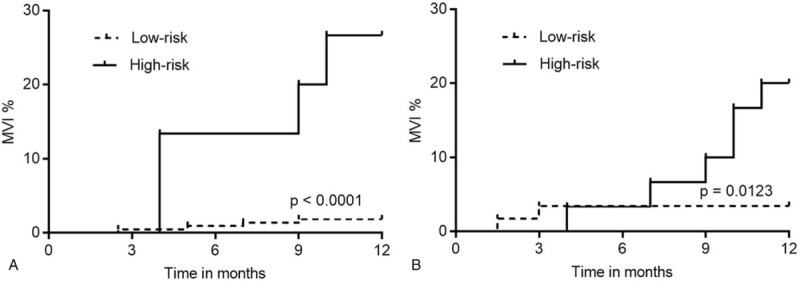
Macroscopic vascular invasion cannot be properly predicted in advance in hepatocellular carcinoma patients based on clinical characteristics and imaging features.To develop a predictive scoring model of macroscopic vascular invasion in hepatocellular carcinoma patients after transcatheter arterial chemoembolization combined with radiofrequency ablation based on specific laboratory and tumor indicators.A predictive scoring model, which estimates the incidence of macroscopic vascular invasion at 1-year follow-up, was constructed based on a derivation cohort of 324 patients with hepatocellular carcinoma; a validation cohort of 120 patients was prospectively included. The prognostic value of the scoring model was determined by concordance index, time-dependent receiver operating characteristics, and calibration curves.Cox multivariate analysis of the derivation cohort identified prothrombin time, aspartate aminotransferase, and Barcelona clinic liver cancer (BCLC) staging as independent predictive factors of macroscopic vascular invasion. The areas under the receiver operating characteristic curves of the predictive scoring model were 0.832 and 0.785 in the derivation and validation cohorts, respectively, and the calibration curves fitted well. Kaplan-Meier analysis showed that the incidence of macroscopic vascular invasion was significantly higher in the high-risk group (score 0-2) than in the low-risk group (score 3-4) in both the derivation and validation cohorts (P < .0001 and P = .0008, respectively).The predictive scoring model enables the accurate prediction of macroscopic vascular invasion incidence 1 year in advance in hepatocellular carcinoma patients who undergo transcatheter arterial chemoembolization combined with radiofrequency ablation.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA: Cancer J Clin 2011;61:69–90. - PubMed
-
- Siegel R, Ma J, Zou Z, et al. Cancer statistics, 2014. CA: Cancer J Clin 2014;64:9–29. - PubMed
-
- Stuart KE, Anand AJ, Jenkins RL. Hepatocellular carcinoma in the United States. Prognostic features, treatment outcome, and survival. Cancer 1996;77:2217–22. - PubMed
-
- Lencioni R, Cioni D, Crocetti L, et al. Early-stage hepatocellular carcinoma in patients with cirrhosis: long-term results of percutaneous image-guided radiofrequency ablation. Radiology 2005;234:961–7. - PubMed
-
- Georgiades CS, Hong K, Geschwind JF. Radiofrequency ablation and chemoembolization for hepatocellular carcinoma. Cancer J 2008;14:117–22. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
