

Man vs machine in emergency medicine - a study on the effects of manual and automatic vital sign documentation on data quality and perceived workload, using observational paired sample data and questionnaires
- PMID: 30545312
- PMCID: PMC6293611
- DOI: 10.1186/s12873-018-0205-2
Man vs machine in emergency medicine - a study on the effects of manual and automatic vital sign documentation on data quality and perceived workload, using observational paired sample data and questionnaires
Abstract
Background: Emergency medicine is characterized by a high patient flow where timely decisions are essential. Clinical decision support systems have the potential to assist in such decisions but will be dependent on the data quality in electronic health records which often is inadequate. This study explores the effect of automated documentation of vital signs on data quality and workload.
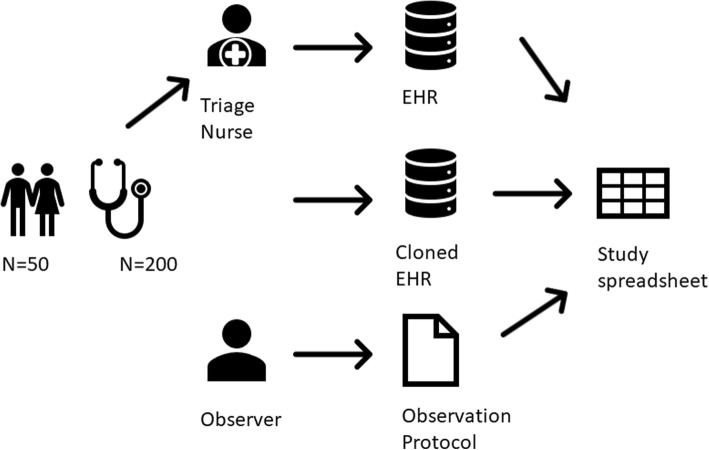
Methods: An observational study of 200 vital sign measurements was performed to evaluate the effects of manual vs automatic documentation on data quality. Data collection using questionnaires was performed to compare the workload on wards using manual or automatic documentation.
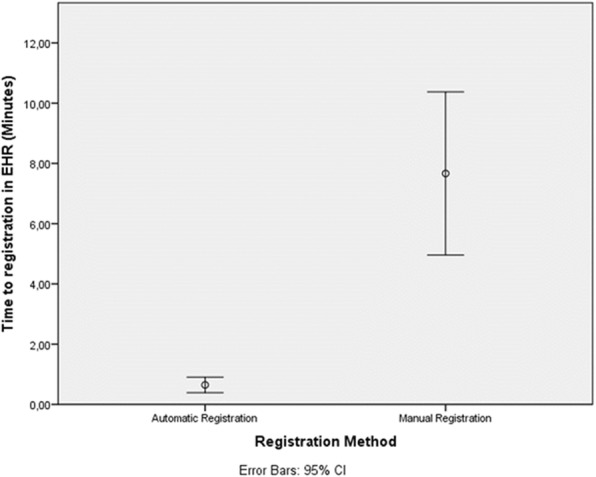
Results: In the automated documentation time to documentation was reduced by 6.1 min (0.6 min vs 7.7 min, p < 0.05) and completeness increased (98% vs 95%, p < 0.05). Regarding workflow temporal demands were lower in the automatic documentation workflow compared to the manual group (50 vs 23, p < 0.05). The same was true for frustration level (64 vs 33, p < 0.05). The experienced reduction in temporal demands was in line with the anticipated, whereas the experienced reduction in frustration was lower than the anticipated (27 vs 54, p < 0.05).
Discussion: The study shows that automatic documentation will improve the currency and the completeness of vital sign data in the Electronic Health Record while reducing workload regarding temporal demands and experienced frustration. The study also shows that these findings are in line with staff anticipations but indicates that the anticipations on the reduction of frustration may be exaggerated among the staff. The open-ended answers indicate that frustration focus will change from double documentation of vital signs to technical aspects of the automatic documentation system.
Keywords: Automated documentation; Data quality; Emergency department; Emergency medicine; Vital signs.
Conflict of interest statement
Ethics approval and consent to participate
All participation of patients and staff was voluntary in the study. Information was given in writing to the participants and they opted in by giving consent to participate in the study. All information was first pseudonymized and later anonymized in the study. Participants were given information on how to withdraw for the study and that such withdrawal was possible to the point where the information was anonymized. An ethical application was granted for the study by the ethical committee in Stockholm (dnr:2014/1207–31/4 and dnr:201/168–31/5).
Consent for publication
No traceable individual data is published in the study.
Competing interests
The main author was appointed as a chief medical officer at the hospital during the study period and one of the researchers is the chief medical informatics officer at the company who delivers the electronic health record system to the hospital.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Musen MA, Middleton B, Greenes RA. Biomedical informatics. London: Springer London; 2014. Clinical decision-support systems; pp. 643–674.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
