

Use of Measures of Inflammation and Kidney Function for Prediction of Atherosclerotic Vascular Disease Events and Death in Patients With CKD: Findings From the CRIC Study
- PMID: 30545708
- PMCID: PMC6812505
- DOI: 10.1053/j.ajkd.2018.09.012
Use of Measures of Inflammation and Kidney Function for Prediction of Atherosclerotic Vascular Disease Events and Death in Patients With CKD: Findings From the CRIC Study
Abstract
Rationale & objective: Traditional risk estimates for atherosclerotic vascular disease (ASVD) and death may not perform optimally in the setting of chronic kidney disease (CKD). We sought to determine whether the addition of measures of inflammation and kidney function to traditional estimation tools improves prediction of these events in a diverse cohort of patients with CKD.
Study design: Observational cohort study.
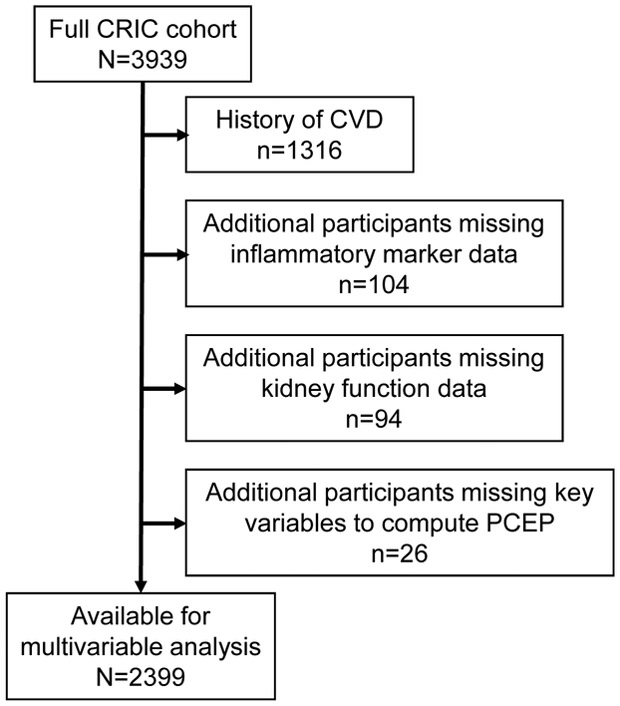
Setting & participants: 2,399 Chronic Renal Insufficiency Cohort (CRIC) Study participants without a history of cardiovascular disease at study entry.
Predictors: Baseline plasma levels of biomarkers of inflammation (interleukin 1β [IL-1β], IL-1 receptor antagonist, IL-6, tumor necrosis factor α [TNF-α], transforming growth factor β, high-sensitivity C-reactive protein, fibrinogen, and serum albumin), measures of kidney function (estimated glomerular filtration rate [eGFR] and albuminuria), and the Pooled Cohort Equation probability (PCEP) estimate.
Outcomes: Composite of ASVD events (incident myocardial infarction, peripheral arterial disease, and stroke) and death.
Analytical approach: Cox proportional hazard models adjusted for PCEP estimates, albuminuria, and eGFR.
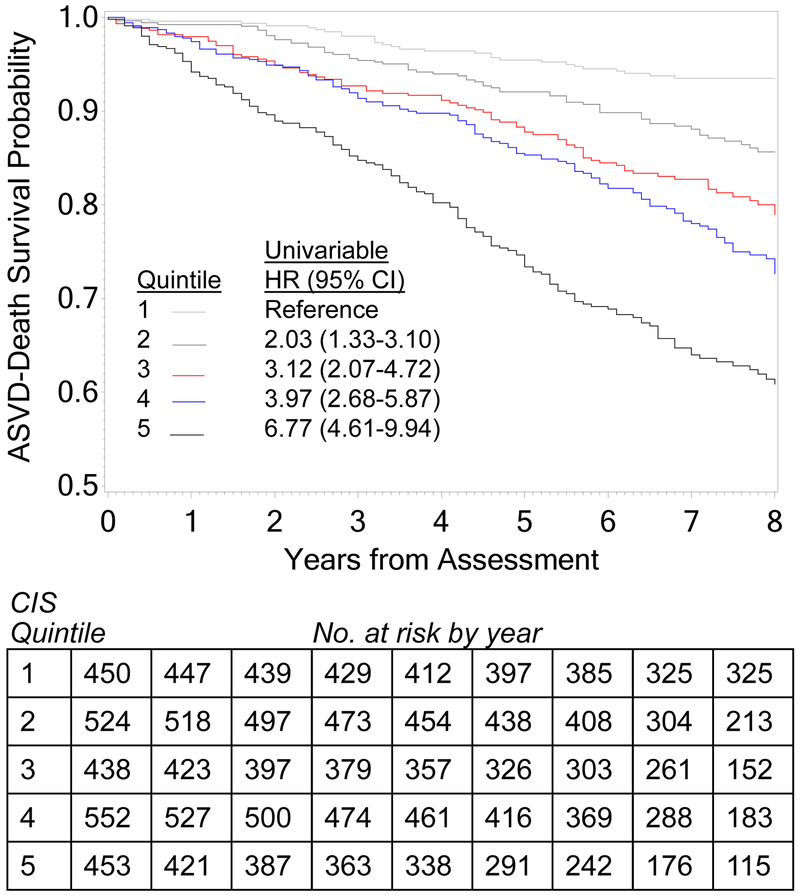
Results: During a median follow-up of 7.3 years, 86, 61, 48, and 323 participants experienced myocardial infarction, peripheral arterial disease, stroke, or death, respectively. The 1-decile greater levels of IL-6 (adjusted HR [aHR], 1.12; 95% CI, 1.08-1.16; P<0.001), TNF-α (aHR, 1.09; 95% CI, 1.05-1.13; P<0.001), fibrinogen (aHR, 1.07; 95% CI, 1.03-1.11; P<0.001), and serum albumin (aHR, 0.96; 95% CI, 0.93-0.99; P<0.002) were independently associated with the composite ASVD-death outcome. A composite inflammation score (CIS) incorporating these 4 biomarkers was associated with a graded increase in risk for the composite outcome. The incidence of ASVD-death increased across the quintiles of risk derived from PCEP, kidney function, and CIS. The addition of eGFR, albuminuria, and CIS to PCEP improved (P=0.003) the area under the receiver operating characteristic curve for the composite outcome from 0.68 (95% CI, 0.66-0.71) to 0.73 (95% CI, 0.71-0.76).
Limitations: Data for cardiovascular death were not available.
Conclusions: Biomarkers of inflammation and measures of kidney function are independently associated with incident ASVD events and death in patients with CKD. Traditional cardiovascular risk estimates could be improved by adding markers of inflammation and measures of kidney function.
Keywords: C-reactive protein (CRP); Myocardial infarction (MI); Pooled Cohort Equation probability (PCEP); albuminuria; atherosclerosis; atherosclerotic vascular disease (ASVD); cardiovascular disease (CVD); chronic kidney function (CKD); cytokines; estimated glomerular filtration rate (eGFR); inflammatory biomarkers; kidney function; risk stratification; stroke.
Copyright © 2018 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ross R Atherosclerosis--an inflammatory disease. New Eng J Medicine 1999;340(2):115–126. - PubMed
-
- Greenland P, Alpert JS, Beller GA et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2010;56(25):e50–103. - PubMed
-
- Stenvinkel P, Heimburger O, Paultre F et al. Strong association between malnutrition, inflammation, and atherosclerosis in chronic renal failure. Kidney Int 1999;55(5):1899–1911. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 TR002548/TR/NCATS NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U01 DK099924/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- R01 DK073665/DK/NIDDK NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- U01 DK099914/DK/NIDDK NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- UL1 TR002003/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
