

Surgical treatment and survival from colorectal cancer in Denmark, England, Norway, and Sweden: a population-based study
- PMID: 30545752
- PMCID: PMC6318222
- DOI: 10.1016/S1470-2045(18)30646-6
Surgical treatment and survival from colorectal cancer in Denmark, England, Norway, and Sweden: a population-based study
Abstract
Background: Survival from colorectal cancer has been shown to be lower in Denmark and England than in comparable high-income countries. We used data from national colorectal cancer registries to assess whether differences in the proportion of patients receiving resectional surgery could contribute to international differences in colorectal cancer survival.
Methods: In this population-based study, we collected data from all patients aged 18-99 years diagnosed with primary, invasive, colorectal adenocarcinoma from Jan 1, 2010, to Dec 31, 2012, in Denmark, England, Norway, and Sweden, from national colorectal cancer registries. We estimated age-standardised net survival using multivariable modelling, and we compared the proportion of patients receiving resectional surgery by stage and age. We used logistic regression to predict the resectional surgery status patients would have had if they had been treated as in the best performing country, given their individual characteristics.
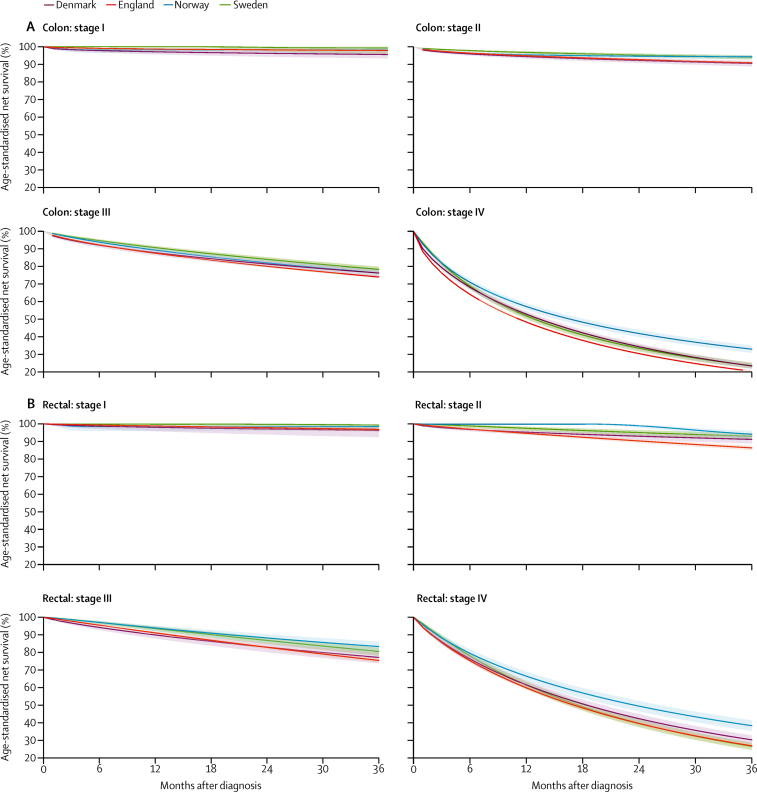
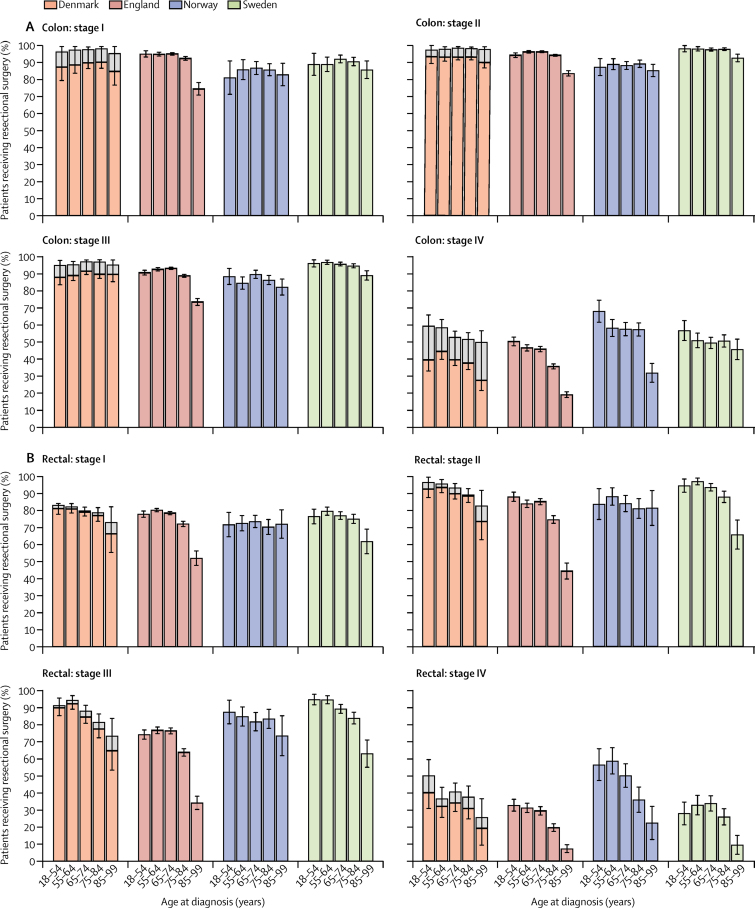
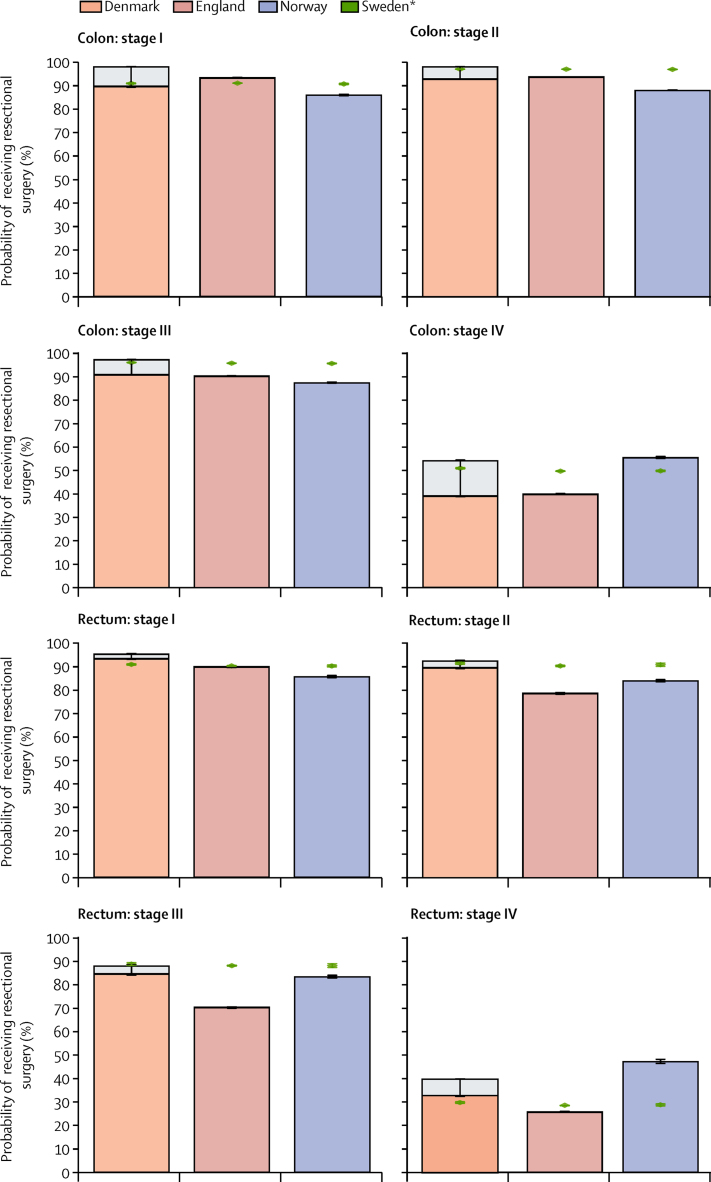
Findings: We extracted registry data for 139 457 adult patients with invasive colorectal adenocarcinoma: 12 958 patients in Denmark, 97 466 in England, 11 450 in Norway, and 17 583 in Sweden. 3-year colon cancer survival was lower in England (63·9%, 95% CI 63·5-64·3) and Denmark (65·7%, 64·7-66·8) than in Norway (69·5%, 68·4-70·5) and Sweden (72·1%, 71·2-73·0). Rectal cancer survival was lower in England (69·7%, 69·1-70·3) than in the other three countries (Denmark 72·5%, 71·1-74·0; Sweden 74·1%, 72·7-75·4; and Norway 75·0%, 73·1-76·8). We found no significant differences in survival for patients with stage I disease in any of the four countries. 3-year survival after stage II or III rectal cancer and stage IV colon cancer was consistently lower in England (stage II rectal cancer 86·4%, 95% CI 85·0-87·6; stage III rectal cancer 75·5%, 74·2-76·7; and stage IV colon cancer 20·5%, 19·9-21·1) than in Norway (94·1%, 91·5-96·0; 83·4%, 80·1-86·1; and 33·0%, 31·0-35·1) and Sweden (92·9%, 90·8-94·6; 80·6%, 78·2-82·7; and 23·7%, 22·0-25·3). 3-year survival after stage II rectal cancer and stage IV colon cancer was also lower in England than in Denmark (stage II rectal cancer 91·2%, 88·8-93·1; and stage IV colon cancer 23·5%, 21·9-25·1). The total proportion of patients treated with resectional surgery ranged from 47 803 (68·4%) of 69 867 patients in England to 9582 (81·3%) of 11 786 in Sweden for colon cancer, and from 16 544 (59·9%) of 27 599 in England to 4106 (70·8%) of 5797 in Sweden for rectal cancer. This range was widest for patients older than 75 years (colon cancer 19 078 [59·7%] of 31 946 patients in England to 4429 [80·9%] of 5474 in Sweden; rectal cancer 4663 [45·7%] of 10 195 in England to 1342 [61·9%] of 2169 in Sweden), and the proportion of patients treated with resectional surgery was consistently lowest in England. The age gradient of the decline in the proportion of patients treated with resectional surgery was steeper in England than in the other three countries in all stage categories. In the hypothetical scenario where all patients were treated as in Sweden, given their age, sex, and disease stage, the largest increase in resectional surgery would be for patients with stage III rectal cancer in England (increasing from 70·3% to 88·2%).
Interpretation: Survival from colon cancer and rectal cancer in England and colon cancer in Denmark was lower than in Norway and Sweden. Survival paralleled the relative provision of resectional surgery in these countries. Differences in patient selection for surgery, especially in patients older than 75 years or individuals with advanced disease, might partly explain these differences in international colorectal cancer survival.
Funding: Early Diagnosis Policy Research Grant from Cancer Research UK (C7923/A18348).
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
The importance of surgery in colorectal cancer treatment.Lancet Oncol. 2019 Jan;20(1):6-7. doi: 10.1016/S1470-2045(18)30679-X. Epub 2018 Dec 10. Lancet Oncol. 2019. PMID: 30545751 No abstract available.
References
-
- International Agency for Research on Cancer GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012. 2015. http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx?cancer=colorectal
-
- Morris EJA, Sandin F, Lambert PC. A population-based comparison of the survival of patients with colorectal cancer in England, Norway and Sweden between 1996 and 2004. Gut. 2011;60:1087–1093. - PubMed
-
- Maringe C, Walters S, Rachet B. Stage at diagnosis and colorectal cancer survival in six high-income countries: a population-based study of patients diagnosed during 2000–7. Acta Oncol. 2013;52:919–932. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
