

An International Analysis of Dialysis Services Reimbursement
- PMID: 30545819
- PMCID: PMC6364535
- DOI: 10.2215/CJN.08150718
An International Analysis of Dialysis Services Reimbursement
Abstract
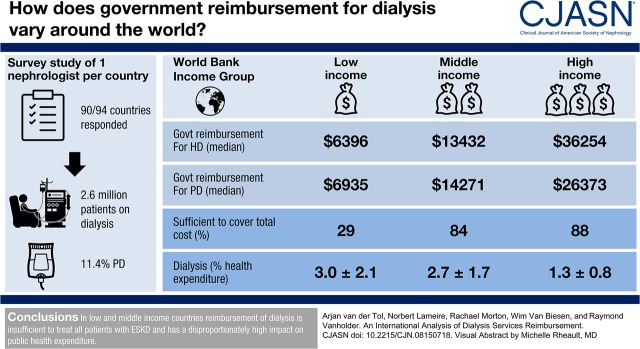
Background and objectives: The prevalence of patients with ESKD who receive extracorporeal kidney replacement therapy is rising worldwide. We compared government reimbursement for hemodialysis and peritoneal dialysis worldwide, assessed the effect on the government health care budget, and discussed strategies to reduce the cost of kidney replacement therapy.
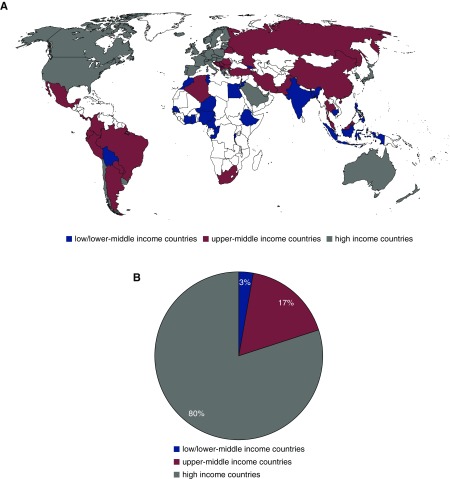
Design, setting, participants, & measurements: Cross-sectional global survey of nephrologists in 90 countries to assess reimbursement for dialysis, number of patients receiving hemodialysis and peritoneal dialysis, and measures to prevent development or progression of CKD, conducted online July to December of 2016.
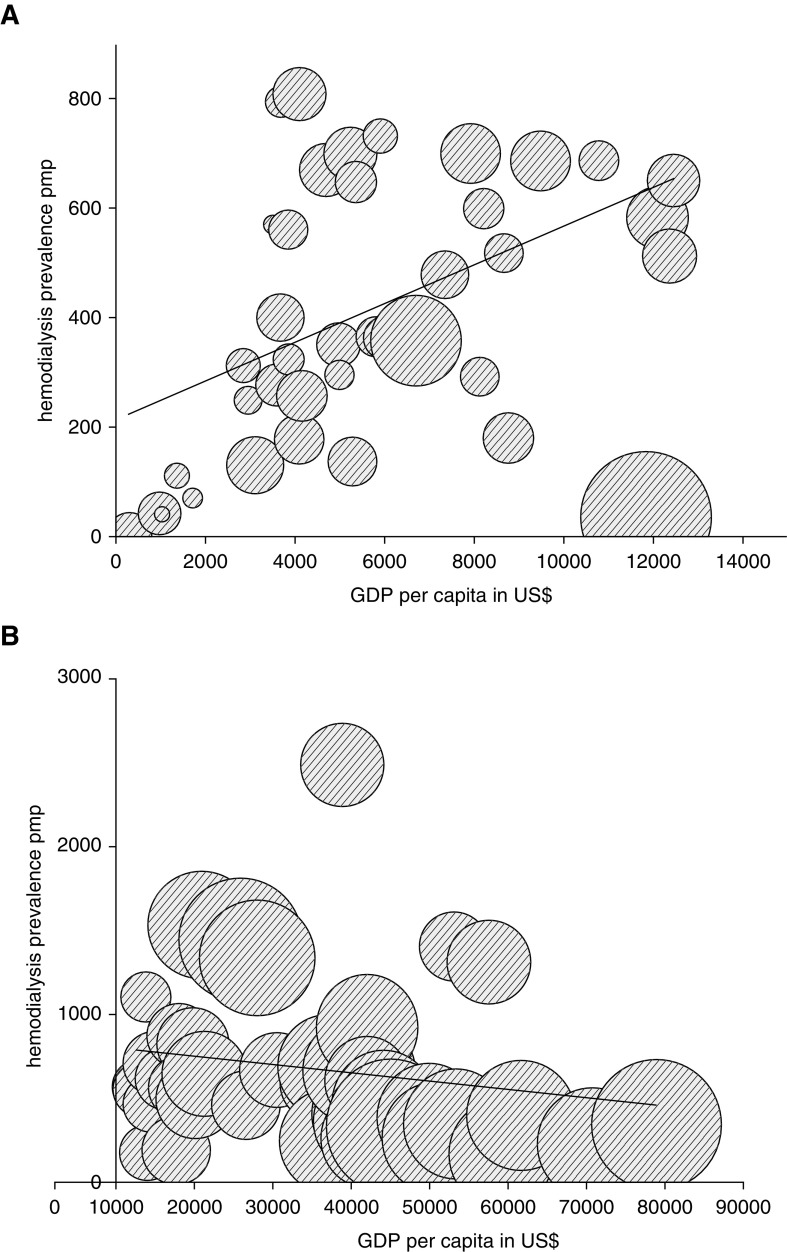
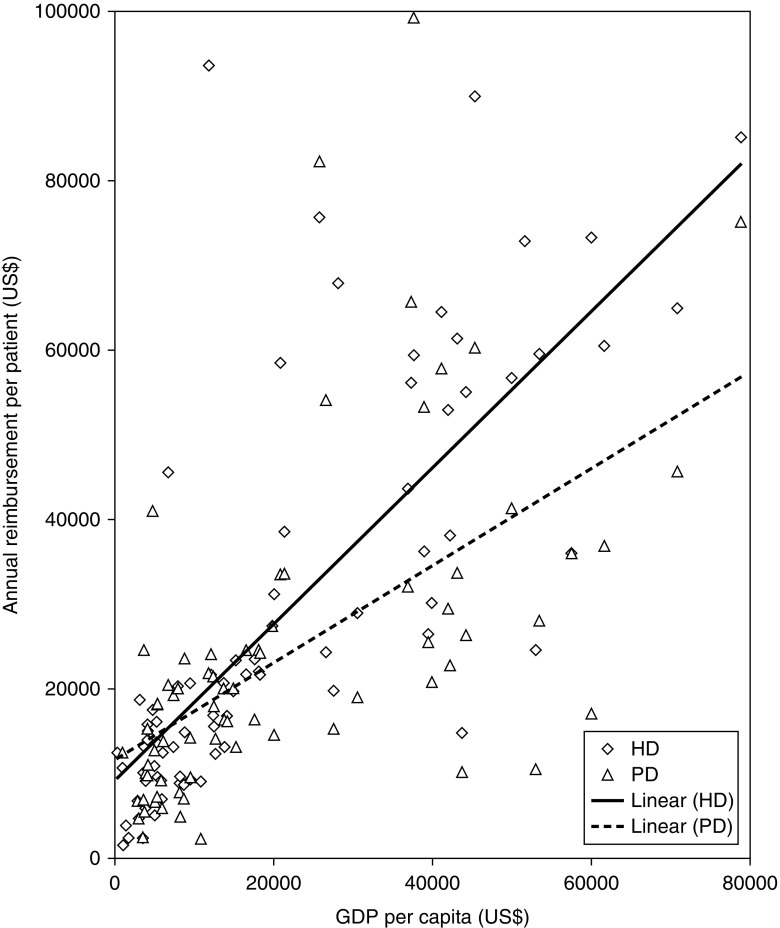
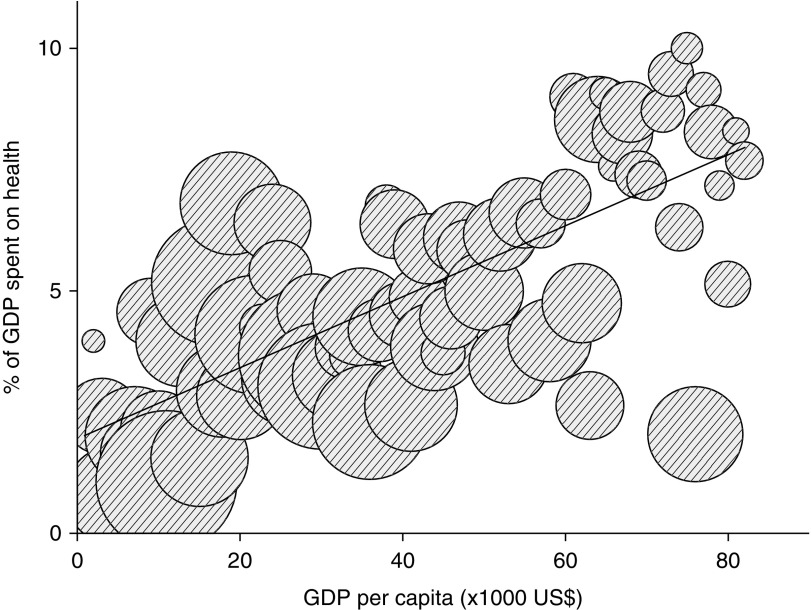
Results: Of the 90 survey respondents, governments from 81 countries (90%) provided reimbursement for maintenance dialysis. The prevalence of patients per million population being treated with long-term dialysis in low- and middle-income countries increased linearly with Gross Domestic Product per capita (GDP per capita), but was substantially lower in these countries compared with high-income countries where we did not observe an higher prevalence with higher GDP per capita. The absolute expenditure for dialysis by national governments showed a positive association with GDP per capita, but the percent of total health care budget spent on dialysis showed a negative association. The percentage of patients on peritoneal dialysis was low, even in countries where peritoneal dialysis is better reimbursed than hemodialysis. The so-called peritoneal dialysis-first policy without financial incentive seems to be effective in increasing the utilization of peritoneal dialysis. Few countries actively provide CKD prevention.
Conclusions: In low- and middle-income countries, reimbursement of dialysis is insufficient to treat all patients with ESKD and has a disproportionately high effect on public health expenditure. Current reimbursement policies favor conventional in-center hemodialysis.
Keywords: chronic dialysis; dialysis health economic; government reimbursement for dialysis services; hemodialysis; peritoneal dialysis; prevalence of dialysis; prevention CKD; worldwide survey.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
-
Influence of Reimbursement Policies on Dialysis Modality Distribution around the World.Clin J Am Soc Nephrol. 2019 Jan 7;14(1):10-12. doi: 10.2215/CJN.13741118. Epub 2018 Dec 13. Clin J Am Soc Nephrol. 2019. PMID: 30545820 Free PMC article. No abstract available.
References
-
- Levin A, Tonelli M, Bonventre J, Coresh J, Donner JA, Fogo AB, Fox CS, Gansevoort RT, Heerspink HJL, Jardine M, Kasiske B, Kottgen A, Kretzler M, Levey AS, Luyckx VA, Mehta R, Moe O, Obrador G, Pannu N, Parikh CR, Perkovic V, Pollock C, Stenvinkel P, Tuttle KR, Wheeler DC, Eckardt KU; ISN Global Kidney Health Summit participants : Global kidney health 2017 and beyond: A roadmap for closing gaps in care, research, and policy. Lancet 390: 1888–1917, 2017 - PubMed
-
- Vanholder R, Lameire N, Annemans L, Van Biesen W: Cost of renal replacement: How to help as many as possible while keeping expenses reasonable? Nephrol Dial Transplant 31: 1251–1261, 2016 - PubMed
-
- Pippias M, Kramer A, Noordzij M, Afentakis N, Alonso de la Torre R, Ambühl PM, Aparicio Madre MI, Arribas Monzón F, Åsberg A, Bonthuis M, Bouzas Caamaño E, Bubic I, Caskey FJ, Castro de la Nuez P, Cernevskis H, de Los Ángeles Garcia Bazaga M, des Grottes JM, Fernández González R, Ferrer-Alamar M, Finne P, Garneata L, Golan E, Heaf JG, Hemmelder MH, Idrizi A, Ioannou K, Jarraya F, Kantaria N, Kolesnyk M, Kramar R, Lassalle M, Lezaic VV, Lopot F, Macario F, Magaz Á, Martín de Francisco AL, Martín Escobar E, Martínez Castelao A, Metcalfe W, Moreno Alia I, Nordio M, Ots-Rosenberg M, Palsson R, Ratkovic M, Resic H, Rutkowski B, Santiuste de Pablos C, Seyahi N, Fernanda Slon Roblero M, Spustova V, Stas KJF, Stendahl ME, Stojceva-Taneva O, Vazelov E, Ziginskiene E, Massy Z, Jager KJ, Stel VS: The European renal association - European dialysis and transplant association registry annual report 2014: A summary. Clin Kidney J 10: 154–169, 2017 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
