

Pulmonary hypertension due to left heart disease
- PMID: 30545974
- PMCID: PMC6351334
- DOI: 10.1183/13993003.01897-2018
Pulmonary hypertension due to left heart disease
Abstract
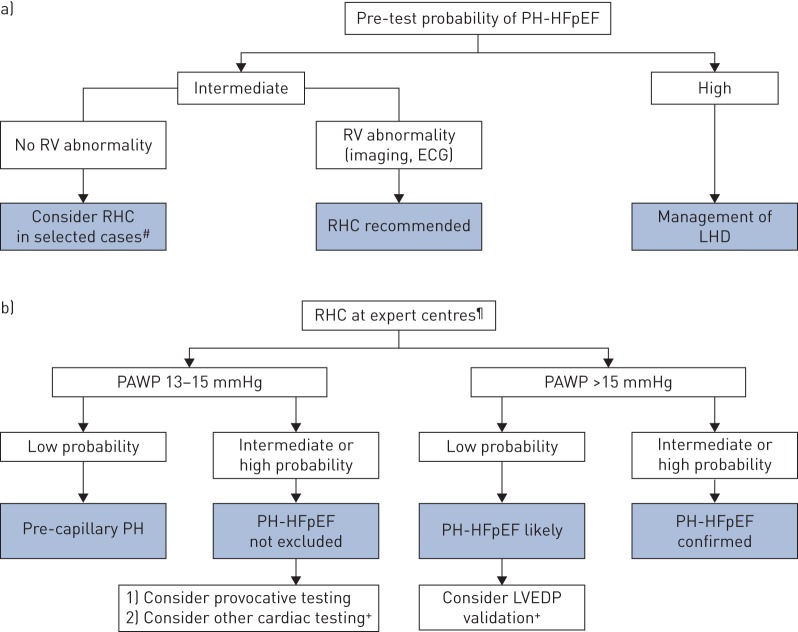
Pulmonary hypertension (PH) is frequent in left heart disease (LHD), as a consequence of the underlying condition. Significant advances have occurred over the past 5 years since the 5th World Symposium on Pulmonary Hypertension in 2013, leading to a better understanding of PH-LHD, challenges and gaps in evidence. PH in heart failure with preserved ejection fraction represents the most complex situation, as it may be misdiagnosed with group 1 PH. Based on the latest evidence, we propose a new haemodynamic definition for PH due to LHD and a three-step pragmatic approach to differential diagnosis. This includes the identification of a specific "left heart" phenotype and a non-invasive probability of PH-LHD. Invasive confirmation of PH-LHD is based on the accurate measurement of pulmonary arterial wedge pressure and, in patients with high probability, provocative testing to clarify the diagnosis. Finally, recent clinical trials did not demonstrate a benefit in treating PH due to LHD with pulmonary arterial hypertension-approved therapies.
Copyright ©ERS 2019.
Conflict of interest statement
Conflict of interest: J-L. Vachiéry reports consultancy and speaker fees paid to institution, and is an investigator in clinical trials for Actelion Pharmaceuticals and Bayer, consultancy fees paid to institution from Novartis, and consultancy fees paid to institution, and is an investigator in clinical trials for Sonivie and Pfizer, during the conduct of the study; consultancy fees paid to institution, and is an investigator in clinical trials for Arena Pharmaceuticals, Bial Portela and Sonivie, consultancy and speaker fees paid to institution, and is an investigator in clinical trials for GSK and Pfizer, consultancy fees and travel grants paid to institution from MSD, and is an investigator in clinical trials for Reata, outside the submitted work. Conflict of interest: R.J. Tedford reports personal fees (Hemodynamic Core Lab) from Actelion, J&J and Merck, and personal fees for steering committee membership from Abbott, outside the submitted work. Conflict of interest: S. Rosenkranz reports personal fees for lectures and/or consultancy from Abbott, Actelion, Arena, Bayer, BMS, MSD, Novartis, Pfizer and United Therapeutics, and institutional research grants from Actelion, Bayer, Novartis, Pfizer and United Therapeutics, outside the submitted work; and serves as chair of the Working Group “Pulmonary circulation and right ventricular function” of the European Society of Cardiology. Conflict of interest: M. Palazzini has nothing to disclose. Conflict of interest: I. Lang reports grants and personal fees from Actelion and AOP Orphan Pharma, and personal fees from Sanofi and Novartis, outside the submitted work. Conflict of interest: M. Guazzi has nothing to disclose. Conflict of interest: G. Coghlan has nothing to disclose. Conflict of interest: I. Chazova has nothing to disclose. Conflict of interest: T. De Marco reports grants from Actelion Pharmaceuticals, Pfizer, United Therapeutics, Gilead, Boston Scientific, Bellerophon, Respirex, Arena Pharmaceutical and Novartis, outside the submitted work.
Figures
Comment in
References
-
- Vachiéry JL, Adir Y, Barbera JA, et al. . Pulmonary hypertension due to left heart diseases. J Am Coll Cardiol 2013; 62: D100–D108. - PubMed
-
- Galiè N, Humbert M, Vachiery JL, et al. . 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J 2015; 46: 903–975. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous