

Pulmonary hypertension in chronic lung disease and hypoxia
- PMID: 30545980
- PMCID: PMC6351338
- DOI: 10.1183/13993003.01914-2018
Pulmonary hypertension in chronic lung disease and hypoxia
Abstract
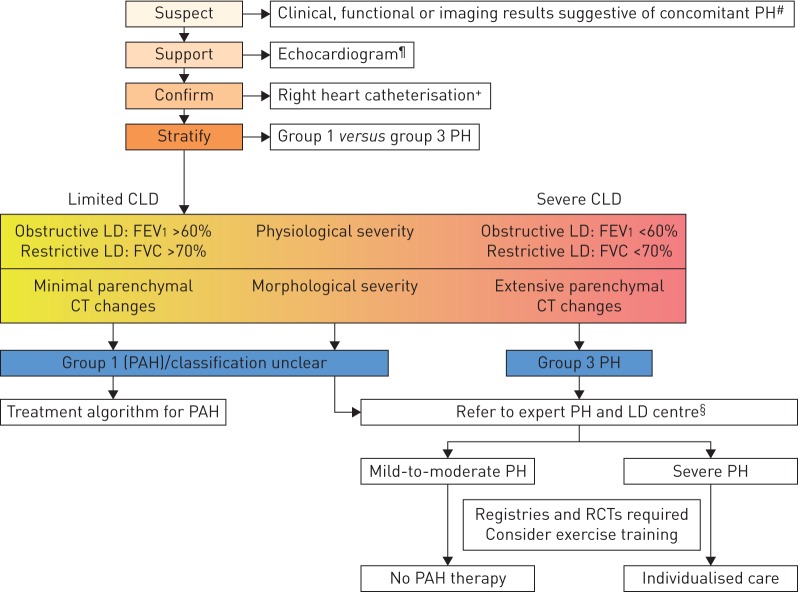
Pulmonary hypertension (PH) frequently complicates the course of patients with various forms of chronic lung disease (CLD). CLD-associated PH (CLD-PH) is invariably associated with reduced functional ability, impaired quality of life, greater oxygen requirements and an increased risk of mortality. The aetiology of CLD-PH is complex and multifactorial, with differences in the pathogenic sequelae between the diverse forms of CLD. Haemodynamic evaluation of PH severity should be contextualised within the extent of the underlying lung disease, which is best gauged through a combination of physiological and imaging assessment. Who, when, if and how to screen for PH will be addressed in this article, as will the current state of knowledge with regard to the role of treatment with pulmonary vasoactive agents. Although such therapy cannot be endorsed given the current state of findings, future studies in this area are strongly encouraged.
Copyright ©ERS 2019.
Conflict of interest statement
Conflict of interest: S.D. Nathan is a consultant for and has received research funding from Bellerophon, United Therapeutics and Bayer Pharmaceuticals; is a consultant for Third Pole and Actelion, and is a consultant for, has received research funding from and is on the speakers’ bureau of Roche-Genentech and Boehringer Ingelheim. Conflict of interest: J.A. Barbera reports grants and personal fees from Actelion and MSD, personal fees from Arena, and grants from Bayer and GSK, outside the submitted work. Conflict of interest: S.P. Gaine reports personal fees from Actelion, United Therapeutics, MSD and GSK, outside the submitted work. Conflict of interest: S. Harari has received grants for research and speakers fees from Actelion, Boehringer Ingelheim and Roche. Conflict of interest: F.J. Martinez has received grants from the NIH (IPF UO1, COPD UO1/RO1); personal fees, honoraria and non-personal travel support from the American College of Chest Physicians, Continuing Education, ConCert, Inova Fairfax Health System, MD Magazine, Miller Communications, National Association for Continuing Education, Novartis, Pearl Pharmaceuticals, PeerView Communications, Prime Communications, Puerto Rican Respiratory Society, Roche, Sunovion, Theravance, Potomac, University of Alabama Birmingham and Zambon; personal fees and non-personal or non-financial travel support from AstraZeneca; personal fees, non-personal travel support, and non-financial support for data and safety monitoring board work from Boehringer Ingelheim; personal fees, honoraria, non-personal travel support, and non-financial support for data and safety monitoring board work from Genentech and GlaxoSmithKline; personal fees and honoraria from Columbia University, Integritas, Methodist Hospital Brooklyn, New York University, Unity, UpToDate, WebMD/MedScape, Western Connecticut Health Network, Academic CME, Patara, PlatformIQ, American Thoracic Society, Rockpointe and Rare Disease Healthcare Communications; non-personal travel support from Nitto; personal fees, honoraria, travel support and non-personal travel support from Chiesi; personal fees, honoraria and travel support from Physicians Education Resource and Teva; honoraria and travel support from Canadian Respiratory Network; personal fees from France Foundation; and has participated on scientific advisory boards (no direct financial compensation) for ProterrixBio and Bridge Biotherapeutics; participated on IPF study steering committees (no direct financial compensation) for Afferent/Merck, Gilead, Veracyte, Prometic, Bayer and ProMedior; and participated on an IPF study steering committee and data safety monitoring board (no direct financial compensation) for Biogen. Conflict of interest: H. Olschewski reports personal fees and non-financial support from Bayer, MSD, Pfizer and Novartis, grants, personal fees and non-financial support from Actelion, grants from Inventiva, and personal fees from Bellerophon, outside the submitted work; and is part-time employee of the Ludwig Boltzmann Institute for Lung Vascular Research. Conflict of interest: K.M. Olsson received fees for talks and consulting work from Actelion, Bayer, GSK, Pfizer and United Therapeutics. Conflict of interest: A.J. Peacock has received research grants and personal fees from Actelion Pharmaceuticals, Bayer, GSK, MSD, Pfizer and United Therapeutics, outside the submitted work. Conflict of interest: J. Pepke-Zaba is a member of the advisory boards for Actelion, Merck, Bayer and GSK, has received grants, personal fees and non-financial support from Actelion, Merck and Bayer, and personal fees from GSK. Conflict of interest: S. Provencher has received research grants from Actelion Pharmaceuticals and Boehringer Ingelheim, and has received speaker fees from Actelion Pharmaceuticals. Conflict of interest: N. Weissmann has nothing to disclose. Conflict of interest: W. Seeger has received consultancy fees from Bayer AG, United Therapeutics, Liquidia, Vectura and Novartis.
Figures
Comment in
References
-
- Seeger W, Adir Y, Barbera JA, et al. Pulmonary hypertension in chronic lung diseases. J Am Coll Cardiol 2013; 62: D109–D116. - PubMed
-
- Medrek SK, Sharafkhaneh A, Spiegelman AM, et al. Admission for COPD exacerbation is associated with the clinical diagnosis of pulmonary hypertension: results from a retrospective longitudinal study of a veteran population. COPD 2017; 14: 484–489. - PubMed
-
- Hayes D Jr, Black SM, Tobias JD, et al. Influence of pulmonary hypertension on patients with idiopathic pulmonary fibrosis awaiting lung transplantation. Ann Thorac Surg 2016; 101: 246–252. - PubMed