

Internal Hernia Associated with Colostomy After Laparoscopic Surgery for Rectal Malignancy: A Report of 3 Thought-Provoking Cases
- PMID: 30546005
- PMCID: PMC6302771
- DOI: 10.12659/AJCR.912676
Internal Hernia Associated with Colostomy After Laparoscopic Surgery for Rectal Malignancy: A Report of 3 Thought-Provoking Cases
Abstract
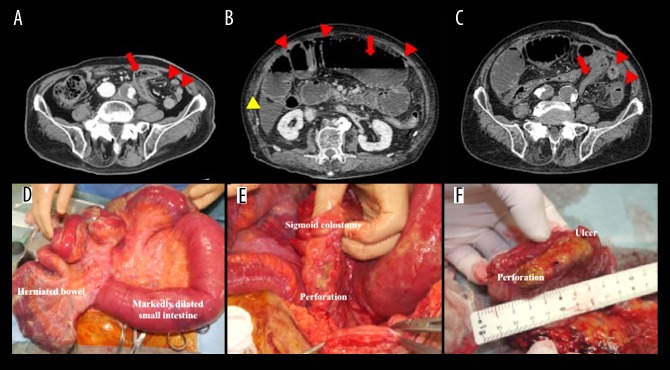
BACKGROUND Colostomy creation via intraperitoneal route is often performed during laparoscopic Hartmann's operation or abdominoperineal resection (APR). Herein, we report 3 rare cases of internal hernia associated with colostomy (IHAC). CASE REPORT The first case involved a 70-year-old man with IHAC after laparoscopic APR. Laparoscopy revealed the small intestine passed through a defect between the lifted sigmoid colon and left lateral abdominal wall in a cranial-to-caudal direction. The dislocated bowel with ischemic change was restored to its normal position and the lateral defect was covered with lateral peritoneum and greater omentum. The second case involved a 75-year-old man with IHAC after laparoscopic APR. Intraperitoneal findings were similar to those in the first case, except for the size of the lateral defect. This defect was too large for primary closure or patching; therefore, no surgical repair was performed. Unfortunately, this led to IHAC recurrence and creation of a new colostomy via extraperitoneal route. The third case involved an 85-year-old man with acute peritonitis resulting from IHAC after laparoscopic Hartmann's operation. Surgery revealed incarcerated bowels forming a closed loop and a perforation in the lifted sigmoid colon. The perforated colon was compressed by the dilated herniated bowel. The resected sigmoid colon showed perforation at the ulcer, which was shown on pathology to be caused by ischemia. CONCLUSIONS IHAC can lead not only to ischemia of strangulated bowel, but also to secondary damage to the lifted colon. During laparoscopic Hartmann's operation or APR, the colostomy should be created via extraperitoneal route to avoid IHAC.
Conflict of interest statement
None.
Figures



References
-
- Scala D, Niglio A, Pace U, et al. Laparoscopic intersphincteric resection: Indications and results. Updates Surg. 2016;68:85–91. - PubMed
-
- Mariani P, Ghanneme A, De la Rochefordiere A, et al. Abdominoperineal resection for anal cancer. Dis Colon Rectum. 2008;51:1495–501. - PubMed
-
- Robertson I, Leung E, Hughes D, et al. Prospective analysis of stoma-related complications. Colorectal Dis. 2005;7:279–85. - PubMed
-
- Xu Z, Guo W. [Clinical research progress of mesenteric internal hernia after Roux-en-Y reconstruction] Zhonghua Wei Chang Wai Ke Za Zhi. 2017;20:352–56. [in Chinese] - PubMed
-
- Toh JW, Lim R, Keshava A, Rickard MJ. The risk of internal hernia or volvulus after laparoscopic colorectal surgery: A systematic review. Colorectal Dis. 2016;18:1133–41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
