

Anchorage possibilities in case of a unilateral maxillary defect using the concept of Strategic Implant®
- PMID: 30546243
- PMCID: PMC6251283
- DOI: 10.4103/njms.NJMS_36_18
Anchorage possibilities in case of a unilateral maxillary defect using the concept of Strategic Implant®
Abstract
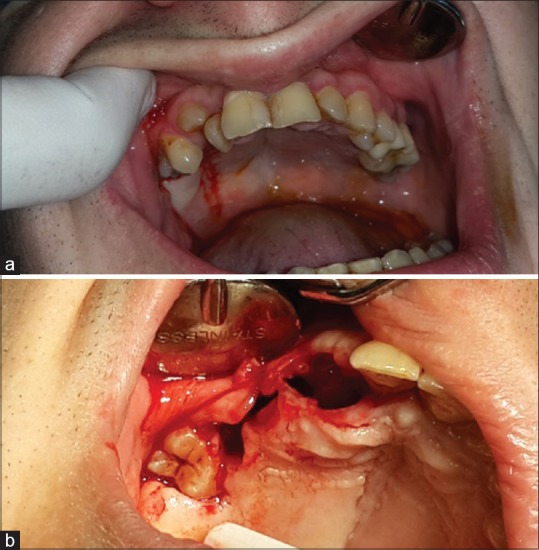
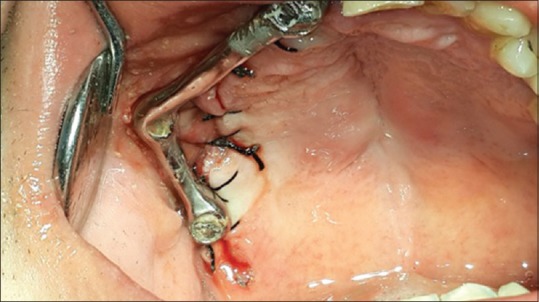
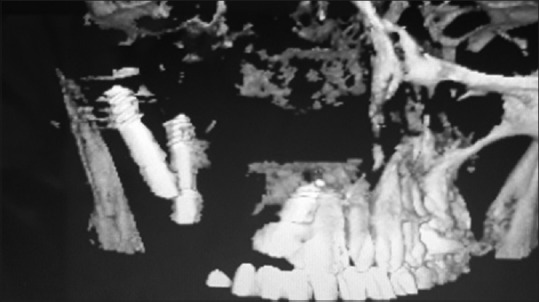
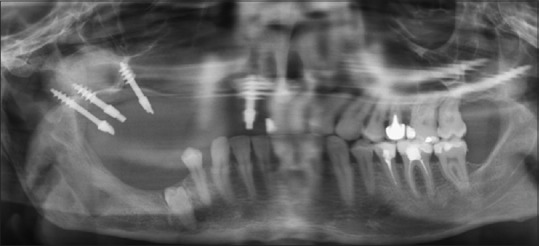
The aim of this article was to present the treatment method applied to a patient who suffered from a multiple fracture of the right maxilla, as a result of an accident that happened to him at an early age. The main consequence of this injury was an inhibited growth of the maxillary bone segment due to the lack of functional stimulus. The treatment consisted of four phases: the removal of all the teeth in the upper right maxilla, the immediate restoration with bicortical implants, the immediate prosthetic rehabilitation, and closing the oroantral communication.
Keywords: Cortical anchorage; Strategic Implant®; immediate loading; maxillary defect; supporting polygon.
Conflict of interest statement
There are no conflicts of interest.
Figures





References
-
- Wolff J. The Law of Bone Remodelling. In: Maquet P, Furlong R, translators. Verlag Von August Hirshwald. Verlag: Springer; 1892.
-
- Frost HM. Wolff's law and bone's structural adaptations to mechanical usage: An overview for clinicians. Angle Orthod. 1994;64:175–88. - PubMed
-
- Hanau RL. Articulation defined, analyzed and formulated. J Am Dent Assoc. 1926;13:1694–709.
-
- Planas P. Equilibrium and neuro-occlusal rehabilitation. Orthod Fr. 1992;63(Pt 2):435–41. - PubMed
-
- Dickerson WG, Chan CA, Carlson J. The human stomatognathic system: A scientific approach to occlusion. Dent Today. 2001;20:100. - PubMed
