

Starfix lead extraction: Clinical experience and technical issues
- PMID: 30546604
- PMCID: PMC6281896
- DOI: 10.1016/j.jccase.2015.09.004
Starfix lead extraction: Clinical experience and technical issues
Abstract
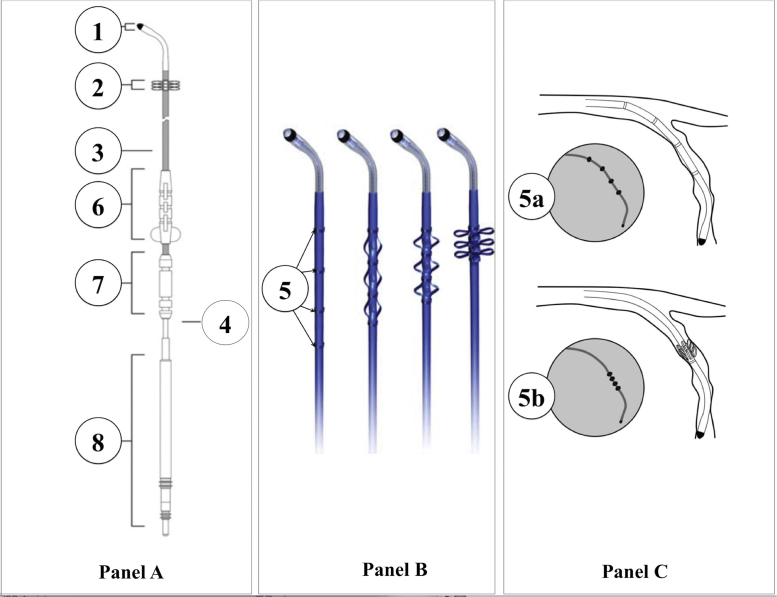
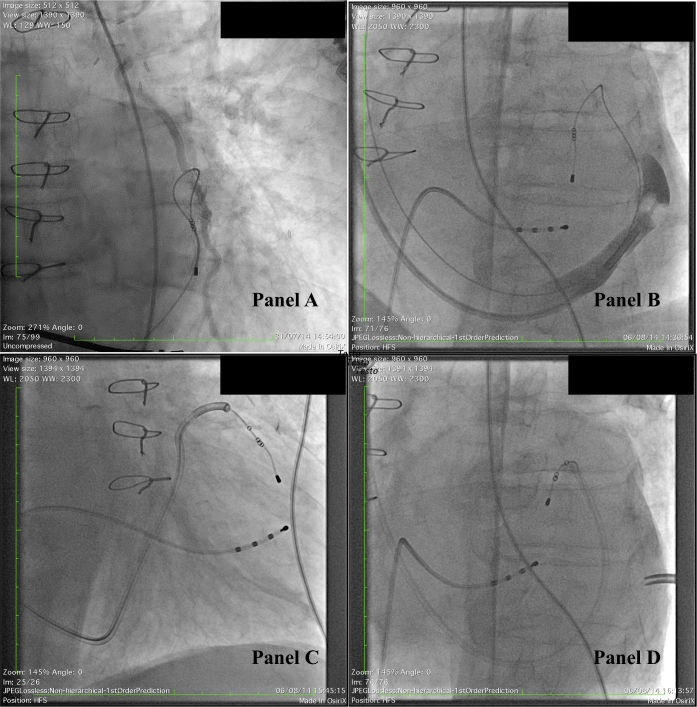
Transvenous lead extraction (TLE) of the Starfix coronary sinus (CS) active-fixation lead may be challenging, due to undeployment of fixation lobes and venous occlusion. We report our experience in Starfix TLE, in comparison with previous data. A 78-year-old male, implanted in 2009 with Starfix lead, was referred to our institution for TLE, due to infective endocarditis with lead-associated vegetations. The tip of Starfix lead was located in distant, anterior position, in the great cardiac vein, close to patent left internal mammary artery-to-left anterior descending artery anastomosis, and first-choice surgical removal had a prohibitive operative risk. Conventional dilatation beyond CS ostium, as well as the use of a standard delivery catheter, was ineffective. An off-label modification of the delivery, by cutting the distal soft tip, was successful. However, the tip of the lead fragmented and was trapped in the innominate vein. Then a gooseneck snare grasped the fragment, allowing complete retrieval. TLE of Starfix leads may be particularly challenging, especially when its tip is located in a distant anterior location. In these cases, important help may be obtained by dilatation within the CS, by means of conventional or modified delivery catheters. Only experienced operators, sometimes with non-conventional techniques, should perform TLE of Starfix leads. <Learning objective: TLE of Starfix leads may be challenging, particularly when the tip is located in a distant anterior position. Dilatation with conventional tools may be precluded. In these cases modifications of the delivery catheters may be useful. Surgery should be avoided as first-choice procedure; only experienced operators, sometimes with non-conventional techniques, should perform TLE of Starfix leads.>.
Keywords: Active-fixation leads; Coronary sinus; Infection; Lead extraction; Starfix lead.
Figures

References
-
- Nagele H., Azizi M., Hashagen S., Castel M.A., Behrens S. First experience with a new active fixation coronary sinus lead. Europace. 2007;9:437–441. - PubMed
-
- Crossley G.H., Exner D., Mead R.H., Sorrentino R.A., Hokanson R., Li S., Adler S. Chronic performance of an active fixation coronary sinus lead. Heart Rhythm. 2010;7:472–478. - PubMed
-
- Wilkoff B.L., Love C.J., Byrd C.L., Bongiorni M.G., Carrillo R.G., Crossley G.H., 3rd, Epstein L.M., Friedman R.A., Kennergren C.E., Mitkowski P., Schaerf R.H., Wazni O.M. Transvenous Lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management: this document was endorsed by the American Heart Association (AHA) Heart Rhythm. 2009;6:1085–1104. - PubMed
-
- Golzio P.G., Gabbarini F., Anselmino M., Vinci M., Gaita F., Bongiorni M.G. Gram-positive occult bacteremia in patients with pacemaker and mechanical valve prosthesis: a difficult therapeutic challenge. Europace. 2010;12:999–1002. - PubMed
-
- Golzio P.G., Manganiello S., Gaita F. Labelled leucocyte scintigraphy in an infected externalized Riata lead. Europace. 2014;16:1442. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
