Review of the Major and Minor Salivary Glands, Part 1: Anatomy, Infectious, and Inflammatory Processes
- PMID: 30546931
- PMCID: PMC6251248
- DOI: 10.4103/jcis.JCIS_45_18
Review of the Major and Minor Salivary Glands, Part 1: Anatomy, Infectious, and Inflammatory Processes
Abstract
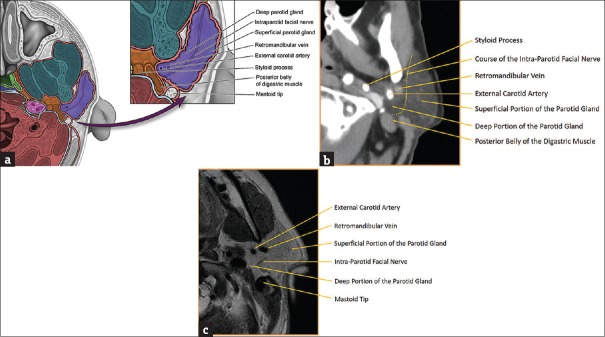
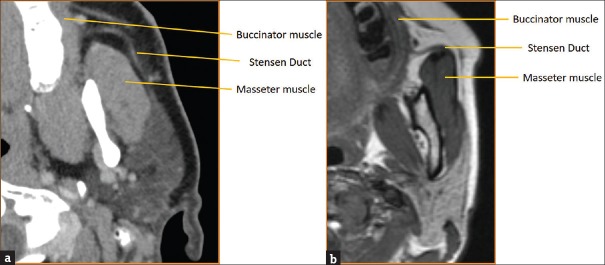
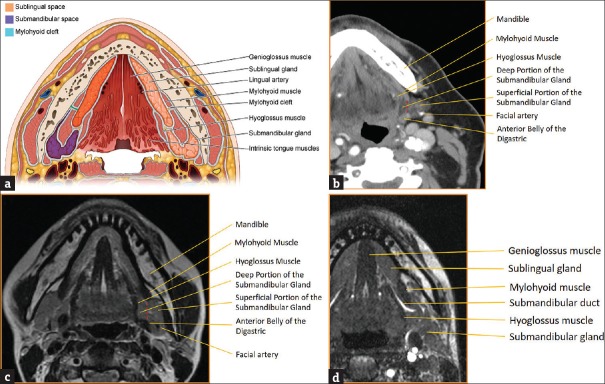
The major and minor salivary glands of the head and neck are important structures that contribute to many of the normal physiologic processes of the aerodigestive tract. The major salivary glands are routinely included within the field of view of standard neuroimaging, and although easily identifiable, salivary pathology is relatively rare and often easy to overlook. Knowledge of the normal and abnormal imaging appearance of the salivary glands is critical for forming useful differential diagnoses, as well as initiating proper clinical workup for what are often incidental findings. The purpose of this review is to provide a succinct image-rich article illustrating relevant anatomy and pathology of the salivary glands via an extensive review of the primary literature. In Part 1, we review anatomy as well as provide an in-depth discussion of the various infectious and inflammatory processes that can affect the salivary glands.
Keywords: Mumps virus; Sjogren's syndrome; salivary gland calculi; salivary glands; sialadenitis.
Conflict of interest statement
There are no conflicts of interest.
Figures

References
-
- Som PM, Brandwin-Gensler MS. Anatomy and pathology of the salivary glands. In: Som PM, Curtin HD, editors. Head and Neck Imaging. 5th ed. St. Louis: Mosby; 2011. pp. 2449–602.
-
- Grossman RI, Yousem DM, editors. Extramucosal diseases of the head and neck. 3rd ed. St. Louis: Mosby; 2010. Neuroradiology: The Requisites; pp. 476–514.
-
- La’porte SJ, Juttla JK, Lingam RK. Imaging the floor of the mouth and the sublingual space. Radiographics. 2011;31:1215–30. - PubMed
-
- Otonari-Yamamoto M, Nakajima K, Tsuji Y, Otonari T, Curtin HD, Okano T, et al. Imaging of the mylohyoid muscle: Separation of submandibular and sublingual spaces. AJR Am J Roentgenol. 2010;194:W431–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources