

Investigating the Association Between Baseline Characteristics (HbA1c and Body Mass Index) and Clinical Outcomes of Fast-Acting Insulin Aspart in People with Diabetes: A Post Hoc Analysis
- PMID: 30547388
- PMCID: PMC6349278
- DOI: 10.1007/s13300-018-0553-7
Investigating the Association Between Baseline Characteristics (HbA1c and Body Mass Index) and Clinical Outcomes of Fast-Acting Insulin Aspart in People with Diabetes: A Post Hoc Analysis
Abstract
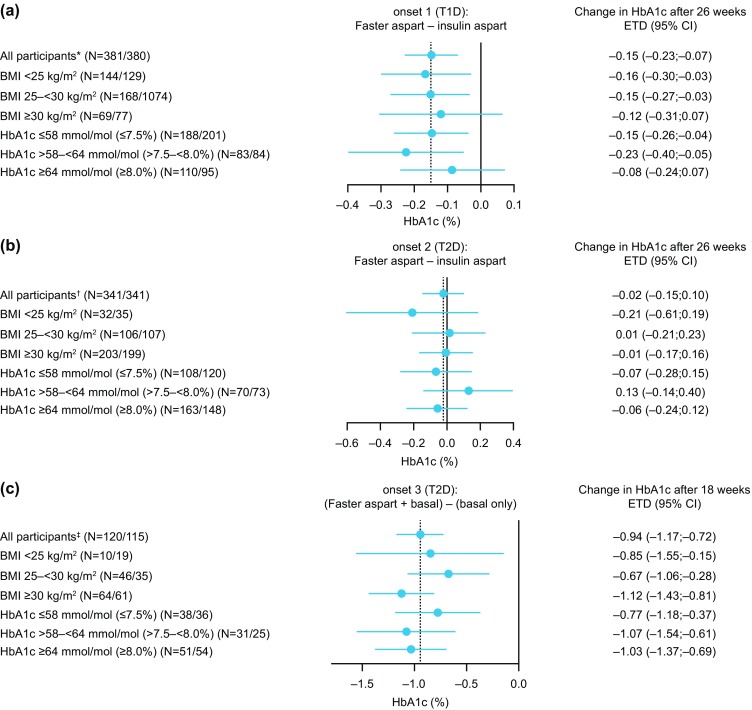
Introduction: The aim of this study was to investigate the association between baseline characteristics [HbA1c and body mass index (BMI)] and the effect of mealtime fast-acting insulin aspart (faster aspart) relative to insulin aspart (IAsp) or basal-only insulin therapy on several efficacy and safety outcomes in people with diabetes.
Methods: Post hoc analysis of three randomised phase 3a trials in people with type 1 diabetes (T1D; onset 1) and type 2 diabetes (T2D; onset 2 and 3). Participants (N = 1686) were stratified according to baseline BMI (< 25 kg/m2, 25-< 30 kg/m2, ≥ 30 kg/m2) or HbA1c (≤ 58 mmol/mol, > 58-< 64 mmol/mol, ≥ 64 mmol/mol; ≤ 7.5%, > 7.5-< 8.0%, ≥ 8.0%).
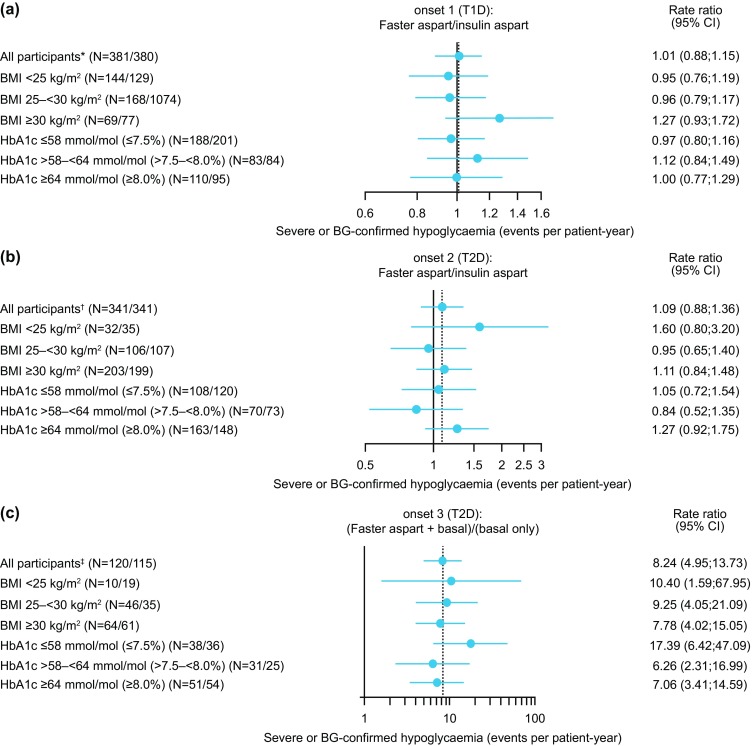
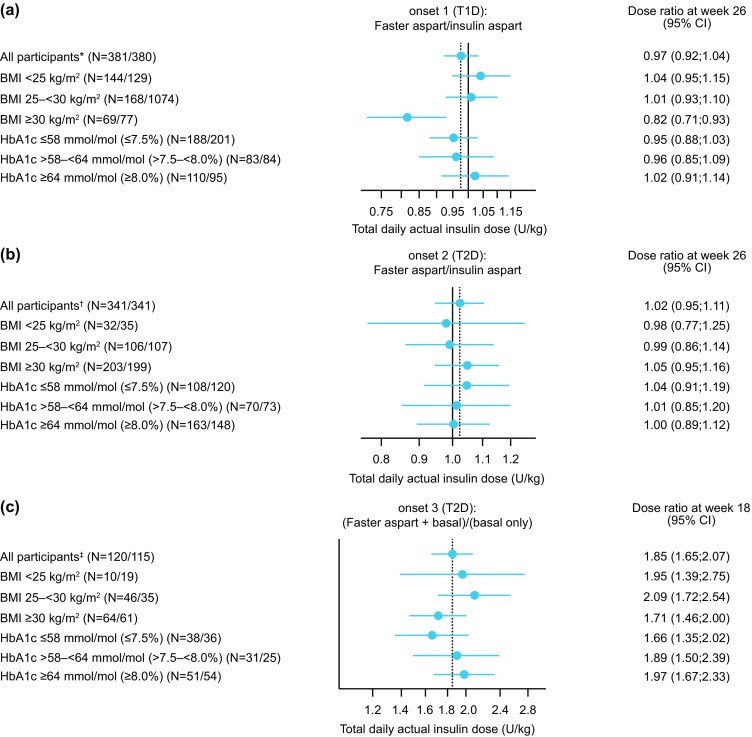
Results: In participants with T2D, the estimated treatment difference for change in HbA1c was similar for all BMI and HbA1c subgroups. No major differences between treatments were observed in risk of overall hypoglycaemia or insulin dose across subgroups. In participants with T1D, change in HbA1c was similar across BMI and HbA1c subgroups, and no major differences between treatments were observed for severe or blood glucose-confirmed hypoglycaemia across subgroups. Total daily insulin dose (U/kg) was similar across all baseline HbA1c groups and the BMI < 25 kg/m2 and 25-30 kg/m2 groups, but was significantly lower with mealtime faster aspart compared with IAsp in the BMI > 30 kg/m2 subgroup.
Conclusions: In participants with T1D and T2D, treatment differences (for change in HbA1c and overall hypoglycaemia) between mealtime faster aspart and insulin comparators were similar to the corresponding overall analysis across baseline HbA1c and BMI subgroups. The finding of a lower total daily insulin dose in participants with obesity (BMI > 30 kg/m2) and T1D treated with faster aspart, versus those treated with IAsp, may warrant further investigation.
Trial registration: ClinicalTrials.gov NCT01831765 (onset 1); NCT01819129 (onset 2); NCT01850615 (onset 3).
Funding: Novo Nordisk A/S, Søborg, Denmark.
Keywords: Diabetes mellitus, type 1; Diabetes mellitus, type 2; Haemoglobin A, glycosylated; Index, body mass; Insulin aspart; Outcome, treatment.
Figures
References
-
- Heise T, Pieber TR, Danne T, Erichsen L, Haahr H. A pooled analysis of clinical pharmacology trials investigating the pharmacokinetic and pharmacodynamic characteristics of fast-acting insulin aspart in adults with type 1 diabetes. Clin Pharmacokinet. 2017;56:551–559. doi: 10.1007/s40262-017-0514-8. - DOI - PMC - PubMed
-
- Russell-Jones D, Bode BW, De Block C, et al. Fast-acting insulin aspart improves glycemic control in basal–bolus treatment for type 1 diabetes: results of a 26-week multicenter, active-controlled, treat-to-target, randomized, parallel-group trial (onset 1) Diabetes Care. 2017;40:943–950. doi: 10.2337/dc16-1771. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
