

Effectiveness and costs of non-invasive foetal RHD genotyping in rhesus-D negative mothers: a French multicentric two-arm study of 850 women
- PMID: 30547830
- PMCID: PMC6295078
- DOI: 10.1186/s12884-018-2114-5
Effectiveness and costs of non-invasive foetal RHD genotyping in rhesus-D negative mothers: a French multicentric two-arm study of 850 women
Abstract
Background: The determination of foetal Rhesus D (RHD) status allows appropriate use of IgRh prophylaxis by restricting its use to cases of RHD feto-maternal incompatibilities. There is a degree of uncertainty about the cost-effectiveness of foetal RHD determination, yet screening programs are being introduced into clinical practice in many countries. This paper evaluates the impact of non-invasive foetal Rhesus D (RHD) status determination on the costs of managing RHD-negative pregnant women and on the appropriate use of anti-D prophylaxis in a large sample of RHD-negative pregnant women using individual prospectively collected clinical and economic data.
Methods: A prospective two-armed trial of RHD negative pregnant women was performed in 11 French Obstetric Departments. Non-invasive foetal RHD genotyping was performed before 26 weeks' gestation in the experimental arm whereas the control arm participants received usual care. The costs associated with patient management in relation to their RHD negative status (biological tests, anti-D prophylaxis and visits) were calculated from inclusion to the end of the postpartum period. The costs of hospital admissions during pregnancy and delivery were also determined.
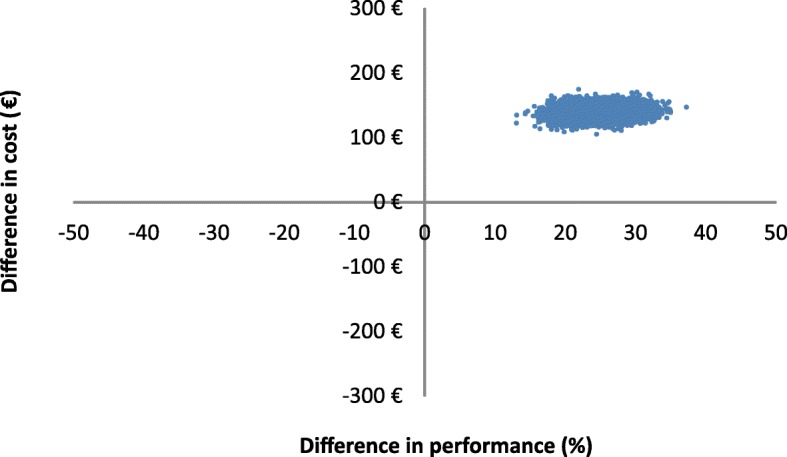
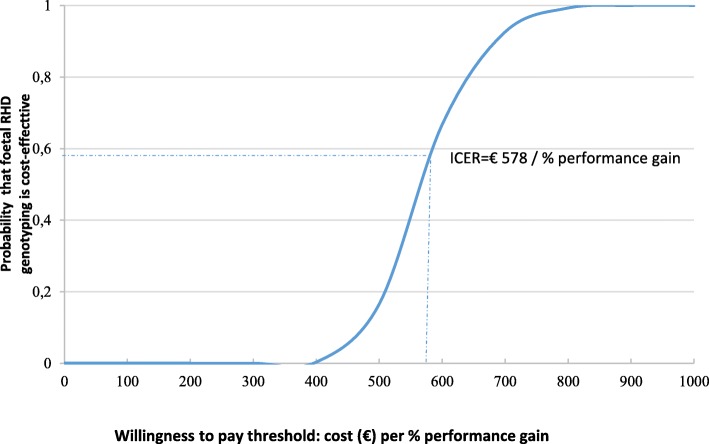
Results: A total of 949 patients were included by 11 centres between 2009 and 2012, and 850 completed follow-up, including medical and biological monitoring. Patients were separated into two groups: the genotyping group (n=515) and the control group (n=335). The cost of the genotyping was estimated at 140 euros per test. The total mean cost per patient was estimated at €3,259 (SD ± 1,120) and €3,004 (SD ± 1,004) in the genotyping and control groups respectively. The cost of delivery represented three quarters of the total cost in both groups. The performance of managing appropriately RHD negative anti-D prophylaxis was 88% in the genotyping group, versus 65% in the control group. Using the costs related to RHD status (biological tests, anti-D immunoglobulin injections and visits) the incremental cost-effectiveness ratio (ICER) was calculated to be €578 for each percentage gain in women receiving appropriate management.
Conclusion: Early knowledge of the RHD status of the foetus using non-invasive foetal RHD genotyping significantly improved the management of RHD negative pregnancies with a small increase in cost.
Trial registration: Clinical trials registry- NCT00832962 -13 January 2009 - retrospectively registered.
Keywords: Anti-D immunoglobulin; Cost evaluation; Cost-effectiveness; Non-invasive foetal RHD genotyping.
Conflict of interest statement
Ethics approval and consent to participate
The ethics committee (Comité de protection des personnes) approved the study. All participants signed an informed consent form. The study was declared to the national committee of computerised records and liberty (Commission Nationale de l’Informatique et des Libertés) before data collection began.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Recommandations pour la pratique clinique 2005. See http://www.cngof.fr (last Accessed 22 May 2017).
-
- National Institute for Health and Care Excellence: High-throughput non-invasive prenatal testing for fetal rhesus D status. Guideline NIHR HTA Programme Technology Assessment Report for NICE DG25; 2016 available from: https://www.nice.org.uk/guidance/dg25
-
- Lo YM, Corbetta N, Chamberlain PF. Presence of fetal DNA in maternal plasma and serum. Lancet. 1997:485–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
