

How Much Blood Could a JP Suck If a JP Could Suck Blood?
- PMID: 30548867
- PMCID: PMC6565520
- DOI: 10.1002/lary.27710
How Much Blood Could a JP Suck If a JP Could Suck Blood?
Abstract
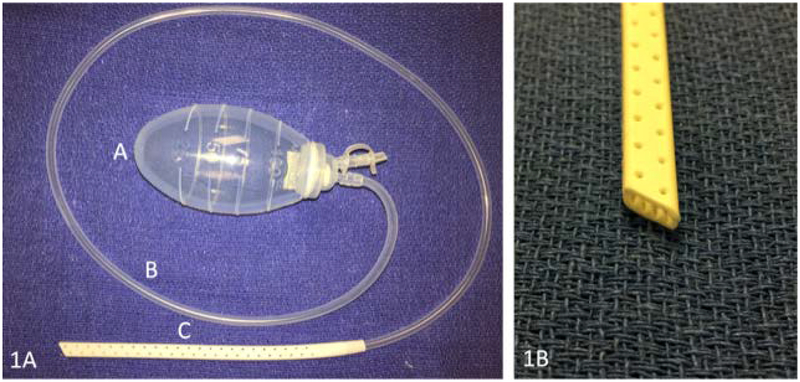
Objective: Active surgical drains minimize fluid accumulation in the postoperative period. The Jackson-Pratt (JP) system consists of a silicone drain connected by flexible tubing to a bulb. When air in the bulb is evacuated, negative pressure is applied at the surgical site to aspirate fluid. The objective of this study was to determine if the evacuation method and volume of accumulated fluid affect the pressure generated by the bulb.
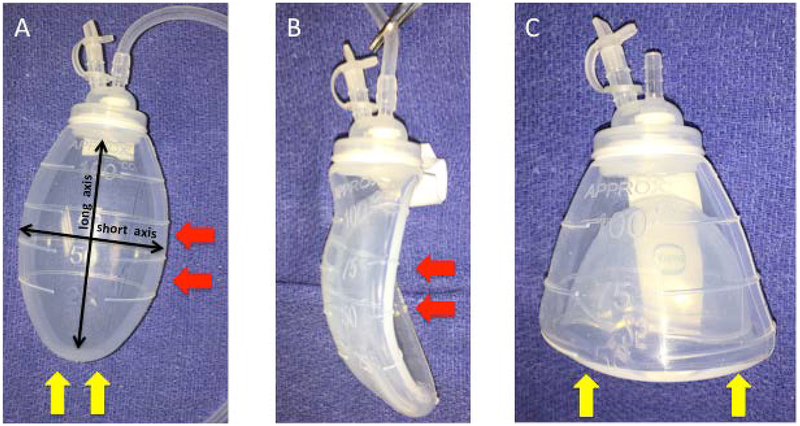
Methods: Bulbs were connected to a digital manometer under various experimental conditions. A random number generator determined the initial evacuation method for each bulb, either side-in or bottom-up. Subsequent evacuations were alternated until data was collected in triplicate for each method. Predetermined amounts of water were placed into the bulb; air was evacuated; and pressure was recorded. The digital manometer was allowed to equilibrate for 1 minute prior to data acquisition.
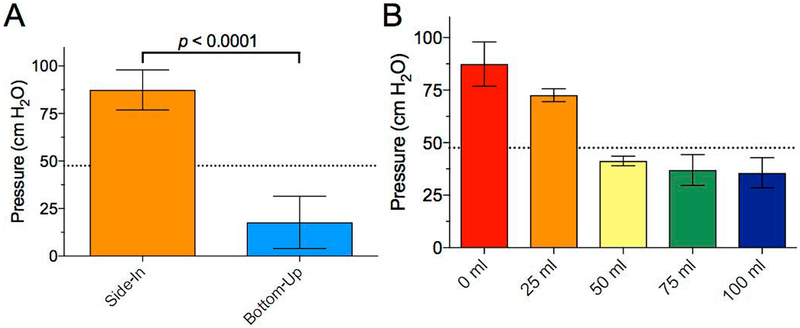
Results: The average amount of pressure after a side-in evacuation of a JP bulb was 87.4 cm H2 O compared to 17.7 cm H2 O for a bottom-up evacuation (P < 0.0001). When the drain contained 25 mL, 50 mL, 75 mL, and 100 mL of fluid, the pressure applied dropped to 72.6, 41.3, 37.0, and 35.6 cm H2 O, respectively.
Conclusions: JP drains generate negative pressure in order to reduce fluid accumulation at surgical sites. Although its function is frequently taken for granted, this study demonstrates that both the specific method for evacuating the bulb as well as the amount of fluid in the bulb significantly affect the performance of this device.
Level of evidence: NA Laryngoscope, 129:1806-1809, 2019.
Keywords: JP drain; Jackson Pratt; surgical drain.
© 2018 The American Laryngological, Rhinological and Otological Society, Inc.
Conflict of interest statement
Conflicts of Interest: No authors have any conflicts of interest.
Figures

References
-
- Zawaneh PN and Putnam D, Materials in surgery: a review of biomaterials in postsurgical tissue adhesion and seroma prevention. Tissue Eng Part B Rev, 2008. 14(4): p. 377–91. - PubMed
-
- Williams J, Toews D, and Prince M, Survey of the use of suction drains in head and neck surgery and analysis of their biomechanical properties. J Otolaryngol, 2003. 32(1): p. 16–22. - PubMed
-
- Durai R and Ng PC, Surgical vacuum drains: types, uses, and complications. Aorn j, 2010. 91(2): p. 266–71; quiz 272–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
