

Persons living with HIV with advanced HIV disease: need for novel care models
- PMID: 30549245
- PMCID: PMC6293147
- DOI: 10.1002/jia2.25210
Persons living with HIV with advanced HIV disease: need for novel care models
Abstract
Introduction: Despite increasing focus on test and treat strategies for people living with HIV (PLHIV), many continue to enrol late in care and initiate antiretroviral therapy (ART) when they have advanced HIV disease.
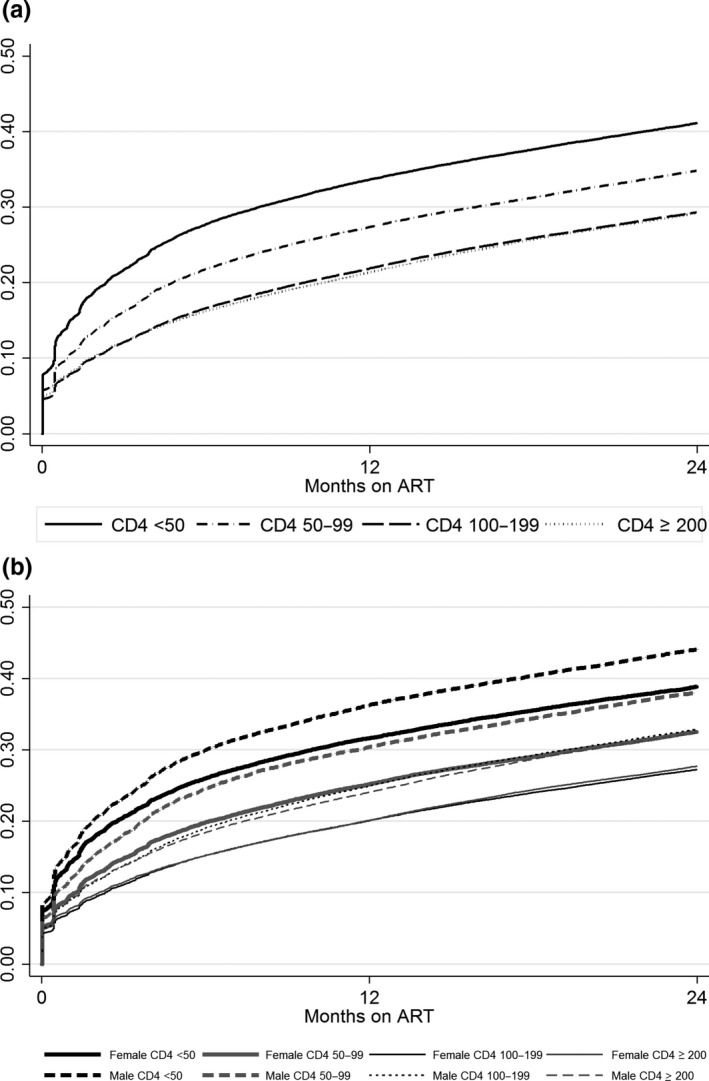
Methods: We analyzed PLHIV ≥15 years of age starting ART in Ethiopia, Kenya, Mozambique and Tanzania from 2005 to 2015 based on CD4+ groups at ART initiation (≥200, 100 to 199, 50 to 99 and <50 cells/mm3 ) to examine attrition (loss to follow-up (LTF) and death) using Kaplan-Meier estimators and Cox proportional hazards models. LTF was defined as no clinic visit >6 months; deaths were ascertained from medical records.
Results and discussion: A total of 305,443 PLHIV were included in the analysis: 118,580 (38.8%) CD4+ ≥200, 91,788 (30.1%) CD4+ 100 to 199, 44,029 (14.4%) CD4+ 50 to 99 and 51,046 (16.7%) CD4+ <50 cells/mm3 . At 12 months after ART initiation, attrition for those with CD4+ ≥200, 100 to 199, 50 to 99 and <50 cells/mm3 was 21.3% (95% CI 21.1 to 21.6), 21.8% (95% CI 21.6 to 22.1), 27.3% (95% CI 26.9 to 27.7) and 33.6% (95% CI 33.2 to 34.0) respectively. In multivariable models, compared to PLHIV with CD4+ ≥200 cells/mm3 , those with CD4+ 50 to 99 cells/mm3 had 29% increased risk of attrition (adjusted hazard ratio (AHR) 1.29, 95% CI 1.27 to 1.32) and those with <50 cells/mm3 had 56% increased risk of attrition (AHR 1.56, 95% CI 1.53 to 1.58). Men had higher attrition compared to women across all CD4+ groups and overall were 28% more likely to experience attrition (AHR 1.28, 95% CI 1.26 to 1.29). Even after ART initiation, PLHIV with advanced disease had notably inferior outcomes with substantial gradient within the low CD4+ strata highlighting the need for targeted interventions for these populations.
Conclusions: Greater efforts, including the identification of effective differentiated service delivery models, are needed to ensure that all PLHIV starting treatment can garner the benefits from ART and achieve favourable outcomes.
Keywords: CD4 cell count; attrition; differentiated service delivery models; late ART initiation; loss to follow-up; mortality.
© 2018 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Figures
References
-
- WHO (World Health Organization) . Guidelines on when to start antiretroviral therapy and on pre‐exposure prophylaxis for HIV. Geneva, Switzerland: WHO; 2015. - PubMed
-
- WHO (World Health Organization) . Treat all: policy adoption and implementation status in countries. Geneva, Switzerland: WHO; 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
