

Estimating the probability of abusive head trauma after abuse evaluation
- PMID: 30551063
- PMCID: PMC6333504
- DOI: 10.1016/j.chiabu.2018.11.015
Estimating the probability of abusive head trauma after abuse evaluation
Abstract
Background: Evidence-based, patient-specific estimates of abusive head trauma probability can inform physicians' decisions to evaluate, confirm, exclude, and/or report suspected child abuse.
Objective: To derive a clinical prediction rule for pediatric abusive head trauma that incorporates the (positive or negative) predictive contributions of patients' completed skeletal surveys and retinal exams.
Participants and setting: 500 acutely head-injured children under three years of age hospitalized for intensive care at one of 18 sites between 2010 and 2013.
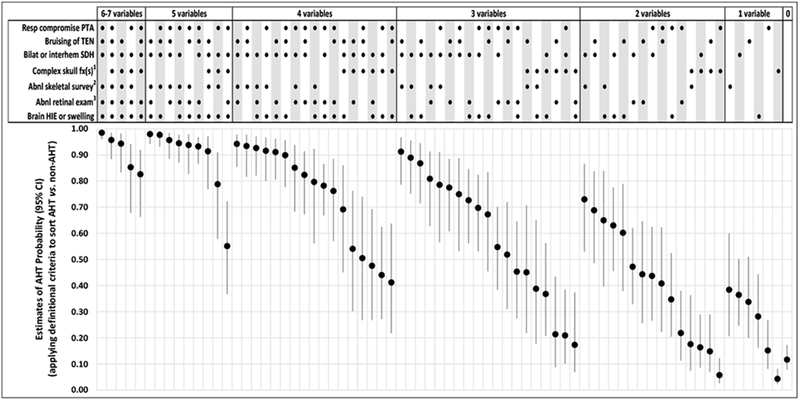
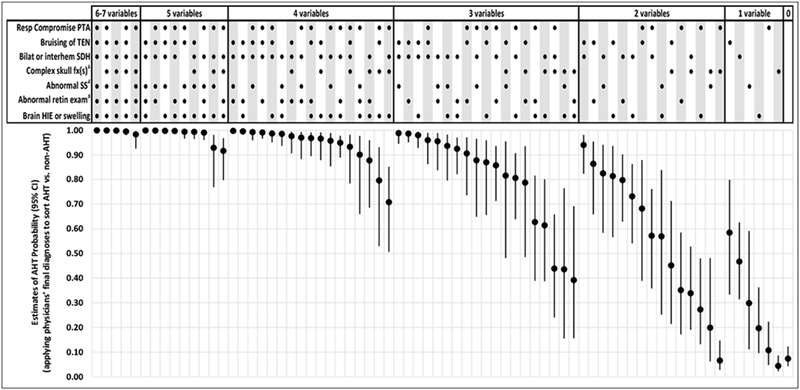
Methods: Secondary analysis of an existing, cross-sectional, prospective dataset, including (1) multivariable logistic regression to impute the results of abuse evaluations never ordered or completed, (2) regularized logistic regression to derive a novel clinical prediction rule that incorporates the results of completed abuse evaluations, and (3) application of the new prediction rule to calculate patient-specific estimates of abusive head trauma probability for observed combinations of its predictor variables.
Results: Applying a mean probability threshold of >0.5 to classify patients as abused, the 7-variable clinical prediction rule derived in this study demonstrated sensitivity 0.73 (95% CI: 0.66-0.79) and specificity 0.87 (95% CI: 0.82-0.90). The area under the receiver operating characteristics curve was 0.88 (95% CI: 0.85-0.92). Patient-specific estimates of abusive head trauma probability for 72 observed combinations of its seven predictor variables ranged from 0.04 (95% CI: 0.02-0.08) to 0.98 (95% CI: 0.96-0.99).
Conclusions: Seven variables facilitate patient-specific estimation of abusive head trauma probability after abuse evaluation in intensive care settings.
Keywords: Abusive head trauma; Child abuse; Clinical prediction rule; Non-accidental trauma; Prediction tool.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures
References
-
- Barlow KM, & Minns RA (2000). Annual incidence of shaken impact syndrome in young children. The Lancet, 356, 1571–1572. - PubMed
-
- Cowley LE, Morris CB, Maguire SA, Farewell DM, & Kemp AM (2015). Validation of a prediction tool for abusive head trauma. Pediatrics, 136, 290–298. - PubMed
-
- Duhaime AC, Alario AJ, Lewander WJ, Schut L, Sutton LN, Seidl TS, Nudelman S, Budenz D, Hertle R, Tsiaras W, & Loporchio S (1992). Head injury in very young children: mechanisms, injury types, and ophthalmologic findings in 100 hospitalized patients younger than 2 years of age. Pediatrics, 90, 179–185. - PubMed
-
- Duhaime AC, Christian CW, Rorke LB, & Zimmerman RA (1998). Nonaccidental head injury in infants--the “shaken-baby syndrome”. New England Journal of Medicine, 338, 1822–1829. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
