

Predicting peripartum blood transfusion in women undergoing cesarean delivery: A risk prediction model
- PMID: 30551126
- PMCID: PMC6294610
- DOI: 10.1371/journal.pone.0208417
Predicting peripartum blood transfusion in women undergoing cesarean delivery: A risk prediction model
Erratum in
-
Correction: Predicting peripartum blood transfusion in women undergoing cesarean delivery: A risk prediction model.PLoS One. 2019 Jan 23;14(1):e0211360. doi: 10.1371/journal.pone.0211360. eCollection 2019. PLoS One. 2019. PMID: 30673777 Free PMC article.
Abstract
Objective: There has been an appreciable rise in postpartum hemorrhage requiring blood transfusions in the United States. Our objective is to better define patients at greatest risk for peripartum transfusion at the time of cesarean in order to identify cases for early intervention and monitoring.
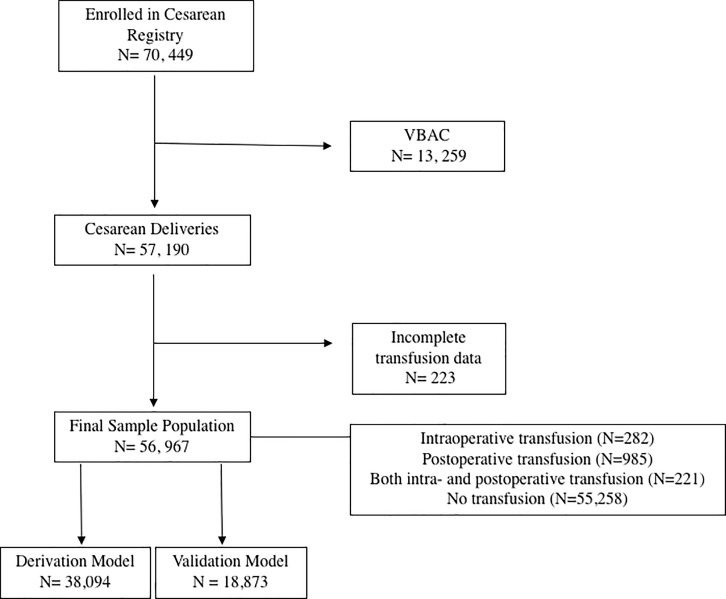
Methods: Our study is a secondary analysis of a retrospective cohort study. Cases of intraoperative and immediate postpartum blood transfusion among women undergoing cesarean delivery were identified. Multivariable logistic regression models were used to identify antepartum and intrapartum risk factors that were independently associated with blood transfusion. A risk calculator was then developed to predict the need for transfusion.
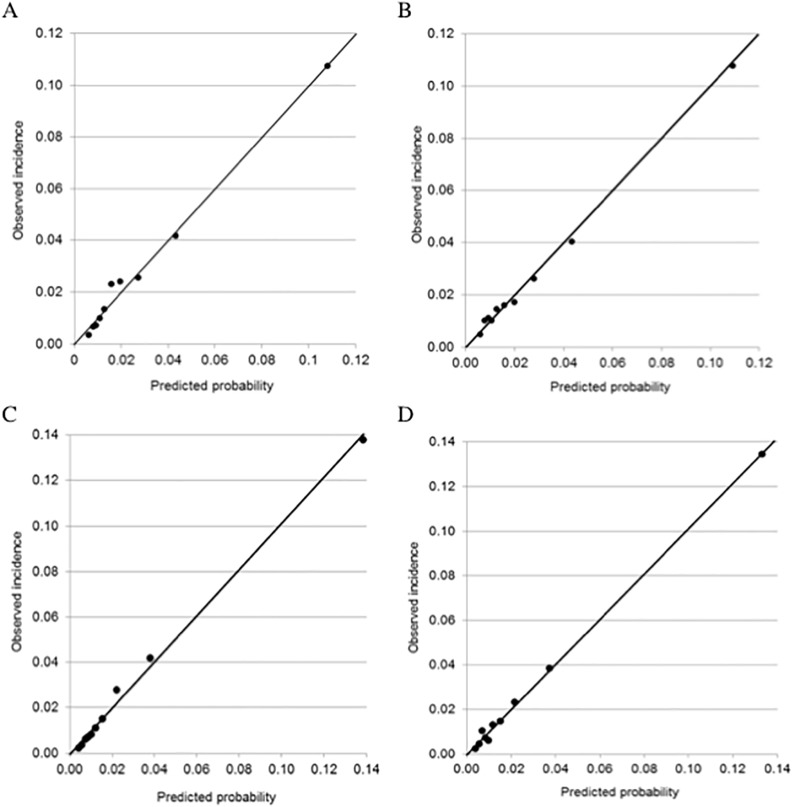
Results: Of 56,967 women, 1488 (2.6%) required any blood transfusion. The strongest risk factors for peripartum blood transfusion included anemia (odds ratio [OR] 3.7, 95% CI 3.3-4.3), abruption on presentation (OR 3.3, CI 2.6-4.1), general anesthesia (OR 5.2, CI 4.4-6.1) and abnormal placentation (OR 92.0, CI 57.4-147.6). An antepartum (model 1) and combined antepartum plus intrapartum risk model (model 2) were developed (model 1 AUC = 0.77, model 2 AUC = 0.83) and internally validated.
Conclusions: Among women who required cesarean delivery, we were able to identify risk factors which predispose women to peripartum blood transfusion and developed a prediction model with good discrimination.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Callaghan WM, Grobman WA, Kilpatrick SJ, Main EK, DʼAlton M. Facility-based identification of women with severe maternal morbidity: it is time to start. Obstet Gynecol. 2014;123: 978–81. 10.1097/AOG.0000000000000218 - DOI - PMC - PubMed
-
- Grobman WA, Bailit JL, Rice MM, Wapner RJ, Reddy UM, Varner MW, et al. Frequency of and factors associated with severe maternal morbidity. Obstet Gynecol. 2014;123: 804–810. 10.1097/AOG.0000000000000173 - DOI - PMC - PubMed
-
- Knight M, Callaghan WM, Berg C, Alexander S, Bouvier-Colle MH, Ford JB, et al. Trends in postpartum hemorrhage in high resource countries: A review and recommendations from the international postpartum hemorrhage collaborative group. Obstet Gynecol Surv. 2010;65: 211–212. 10.1097/01.ogx.0000371705.17102.c4 - DOI - PMC - PubMed
-
- McLintock C, James AH. Obstetric hemorrhage. J Thromb Haemost. 2011;9: 1441–1451. 10.1111/j.1538-7836.2011.04398.x - DOI - PubMed
-
- World Health Organization. WHO recommendations for the prevention and treatment of postpartum haemorrhage [Internet]. 2012. Available: http://www.who.int/reproductivehealth/publications/maternal_perinatal_he... - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
