

Medical Service Quality, Efficiency and Cost Control Effectiveness of Upgraded Case Payment in Rural China: A Retrospective Study
- PMID: 30551561
- PMCID: PMC6313562
- DOI: 10.3390/ijerph15122839
Medical Service Quality, Efficiency and Cost Control Effectiveness of Upgraded Case Payment in Rural China: A Retrospective Study
Abstract
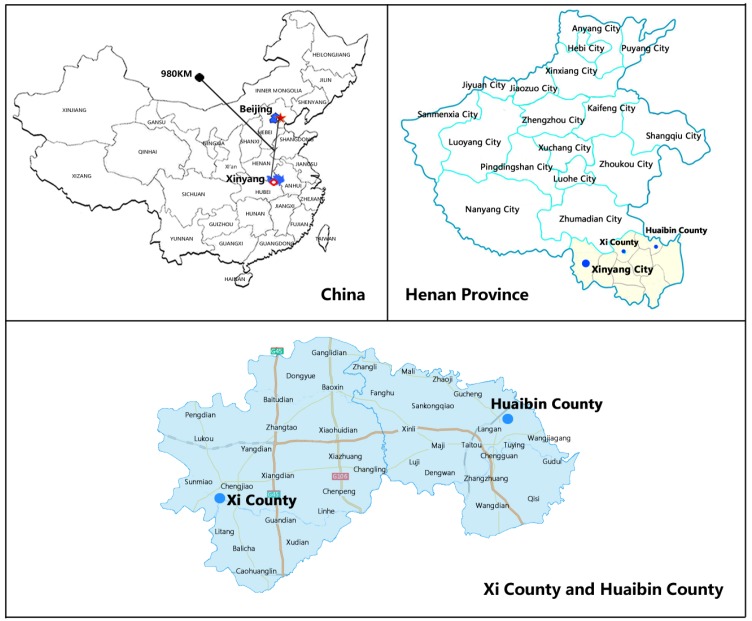
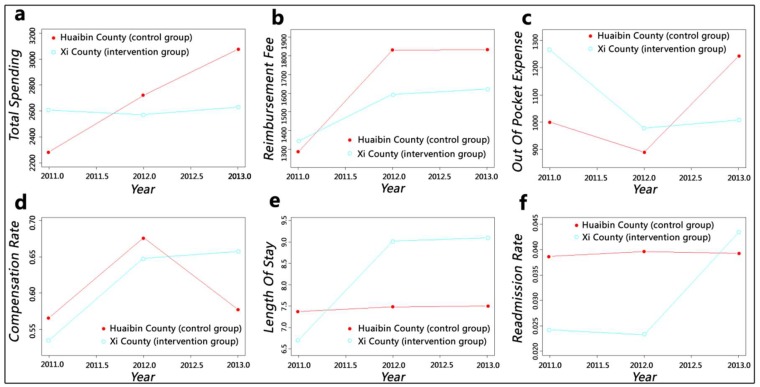
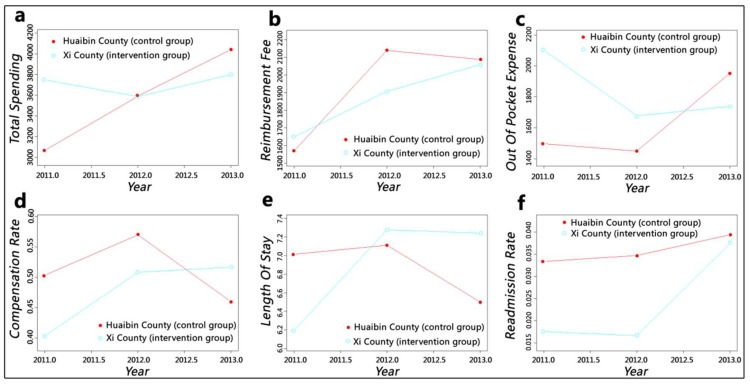
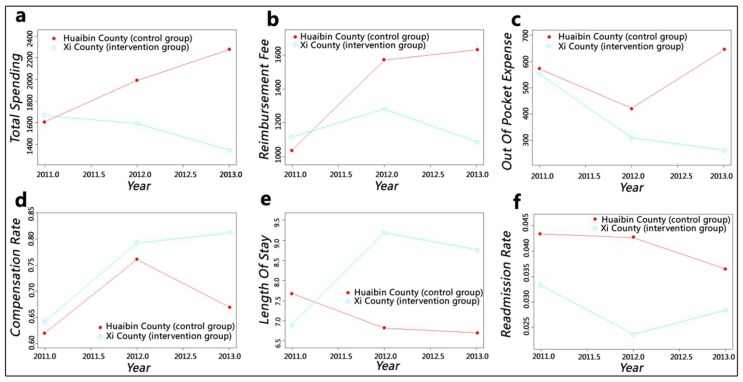
Background: As the principal means of reimbursing medical institutions, the effects of case payment still need to be evaluated due to special environments and short exploration periods, especially in rural China. Methods: Xi County was chosen as the intervention group, with 36,104, 48,316, and 59,087 inpatients from the years 2011 to 2013, respectively. Huaibin County acted as the control group, with 33,073, 48,122, and 51,325 inpatients, respectively, from the same period. The inpatients' information was collected from local insurance agencies. After controlling for age, gender, institution level, season fixed effects, disease severity, and compensation type, the generalised additive models (GAMs) and difference-in-differences approach (DID) were used to measure the changing trends and policy net effects from two levels (the whole county level and each institution level) and three dimensions (cost, quality and efficiency). Results: At the whole-county level, the cost-related indicators of the intervention group showed downward trends compared to the control group. Total spending, reimbursement fee and out-of-pocket expense declined by ¥346.59 (p < 0.001), ¥105.39 (p < 0.001) and ¥241.2 (p < 0.001), respectively (the symbol ¥ represents Chinese yuan). Actual compensation ratio, length of stay, and readmission rates exhibited ascending trends, with increases of 7% (p < 0.001), 2.18 days (p < 0.001), and 1.5% (p < 0.001), respectively. The intervention group at county level hospital had greater length of stay reduction (¥792.97 p < 0.001) and readmission rate growth (3.3% p < 0.001) and lower reimbursement fee reduction (¥150.16 p < 0.001) and length of stay growth (1.24 days p < 0.001) than those at the township level. Conclusions: Upgraded case payment is more reasonable and suitable for rural areas than simple quota payment or cap payment. It has successfully curbed the growth of medical expenses, improved the efficiency of medical insurance fund utilisation, and alleviated patients' economic burden of disease. However, no positive effects on service quality and efficiency were observed. The increase in readmission rate and potential hidden dangers for primary health care institutions should be given attention.
Keywords: case payment; cost control; efficiency; quality; rural China; upgraded version.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- OECD Health at a Glance 2017: OECD Indicators. [(accessed on 10 November 2017)];2017 doi: 10.1787/health_glance-2017-en. Available online: - DOI
-
- National Health and Family Planning Commission of the People’s Republic of China China Health Statistical Yearbook 2017. [(accessed on 1 September 2017)]; Available online: http://www.yearbookchina.com/navibooklist-n2017120225-1.html. (In Chinese)
-
- Eggleston K. Kan Bing Nan, Kan Bing Gui: Challenges for China’s Healthcare System Thirty Years into Reform. Walter, H. Shorenstein Asia-Pacific Research Center; Stanford, CA, USA: 2010.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
