

Direct-Acting Antivirals in Hepatitis C Virus-Associated Diffuse Large B-cell Lymphomas
- PMID: 30552159
- PMCID: PMC6693710
- DOI: 10.1634/theoncologist.2018-0331
Direct-Acting Antivirals in Hepatitis C Virus-Associated Diffuse Large B-cell Lymphomas
Abstract
Background: International guidelines suggest hepatitis C virus (HCV) eradication by direct-acting antivirals (DAAs) after first-line immunochemotherapy (I-CT) in patients with HCV-positive diffuse large B-cell lymphoma (DLBCL), although limited experiences substantiate this recommendation. Moreover, only a few data concerning concurrent administration of DAAs with I-CT have been reported.
Subjects, materials, and methods: We analyzed hematological and virological outcome and survival of 47 consecutive patients with HCV-positive DLBCL treated at 23 Italian and French centers with DAAs either concurrently (concurrent cohort [ConC]: n = 9) or subsequently (sequential cohort [SeqC]: n = 38) to first-line I-CT (mainly rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone [R-CHOP]-like).
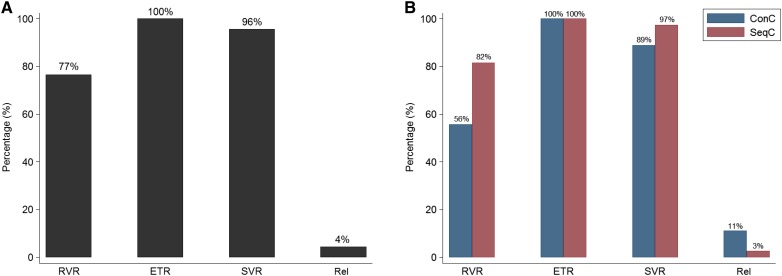
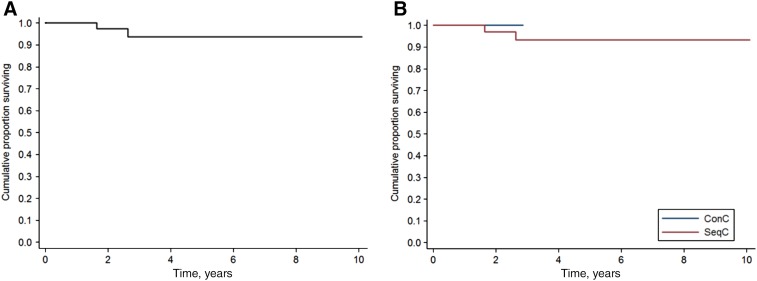
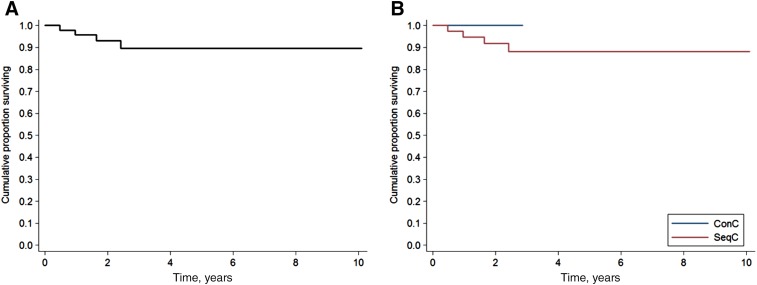
Results: Median age was 61 years, 89% of patients had stage III/IV, and 25% presented evidence of cirrhosis. Genotype was 1 in 56% and 2 in 34% of cases. Overall, 46 of 47 patients obtained complete response to I-CT. All patients received appropriate DAAs according to genotype, mainly sofosbuvir-based regimens (n = 45). Overall, 45 patients (96%) achieved sustained virological response, 8 of 9 in ConC and 37 of 38 in SeqC. DAAs were well tolerated, with only 11 patients experiencing grade 1-2 adverse events. Twenty-three patients experienced hepatic toxicity (grade 3-4 in seven) following I-CT in SeqC, compared to only one patient in ConC. At a median follow-up of 2.8 years, two patients died (2-year overall survival, 97.4%) and three progressed (2-year progression-free survival, 93.1%).
Conclusion: Excellent outcome of this cohort of HCV-positive DLBCL suggests benefit of HCV eradication by DAAs either after or during I-CT. Moreover, concurrent DAAs and R-CHOP administration appeared feasible, effective, and ideally preferable to deferred administration of DAAs for the prevention of hepatic toxicity.
Implications for practice: Hepatitis C virus (HCV)-associated diffuse large B-cell lymphomas (DLBCLs) represent a great therapeutic challenge, especially in terms of hepatic toxicity during immune-chemotherapy (I-CT) and long-term hepatic complications. The advent of highly effective and toxicity-free direct-acting antivirals (DAAs) created an exciting opportunity to easily eradicate HCV shortly after or in concomitance with first-line immunochemotherapy (usually R-CHOP). This retrospective international study reports the real-life use of the combination of these two therapeutic modalities either in the concurrent or sequential approach (DAAs after I-CT) in 47 patients. The favorable reported results on long-term outcome seem to support the eradication of HCV with DAAs in all patients with HCV-positive DLBCL. Moreover, the results from the concurrent approach were effective and safe and displayed an advantage in preventing hepatic toxicity during I-CT.
Keywords: Diffuse large B‐cell lymphoma; Direct‐acting antivirals; Hepatitis C virus; R‐CHOP.
© AlphaMed Press 2018.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Mele A, Pulsoni A, Bianco E et al. Hepatitis C virus and b‐cell non‐Hodgkin lymphomas: An Italian multicenter case‐control study. Blood 2003;102:996–999. - PubMed
-
- Arcaini L, Pascutto C, Passamonti F et al. Bayesian models identify specific lymphoproliferative disorders associated with hepatitis C virus infection. Int J Cancer 2009;124:2246–2249. - PubMed
-
- Nieters A, Kallinowski B, Brennan P et al. Hepatitis C and risk of lymphoma: Results of the European multicenter case‐control study EPILYMPH. Gastroenterology 2006;131:1879–1886. - PubMed
