

Implications of secondary aortic intervention after thoracic endovascular aortic repair for acute and chronic type B dissection
- PMID: 30553732
- PMCID: PMC6478524
- DOI: 10.1016/j.jvs.2018.07.080
Implications of secondary aortic intervention after thoracic endovascular aortic repair for acute and chronic type B dissection
Abstract
Background: Thoracic endovascular aortic repair (TEVAR) has become a mainstay of therapy for acute and chronic type B aortic dissection (TBAD). Dynamic aortic morphologic changes, untreated dissected aorta, and persistent false lumen perfusion have significant consequences for reintervention after TEVAR for TBAD. However, few reports contrast differences in secondary aortic intervention (SAI) after TEVAR for TBAD or describe their influence on mortality. This analysis examined incidence, timing, and types of SAI after TEVAR for acute and chronic TBAD and determined their impact on survival.
Methods: All TEVAR procedures for acute and chronic TBAD (2005-2016) were retrospectively reviewed. Patients with staged (<30 days) or concomitant ascending aortic arch repair or replacement were excluded. Acuity was defined by symptom onset (0-30 days, acute; >30 days, chronic). SAI procedures were grouped into open (intended treatment zone or remote aortic site), major endovascular (TEVAR extension or endograft implanted at noncontiguous site), and minor endovascular (side branch or false lumen embolization) categories. Kaplan-Meier methodology was used to estimate freedom from SAI and survival. Cox proportional hazards were used to identify SAI predictors.
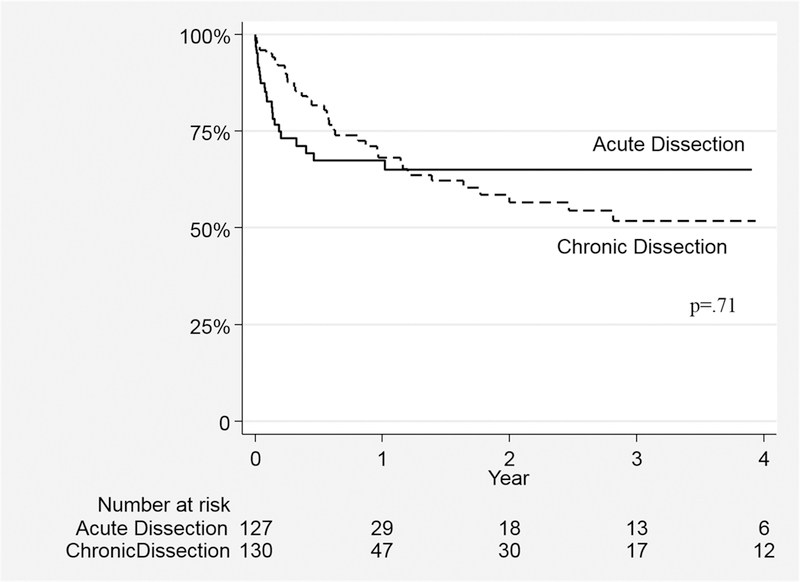
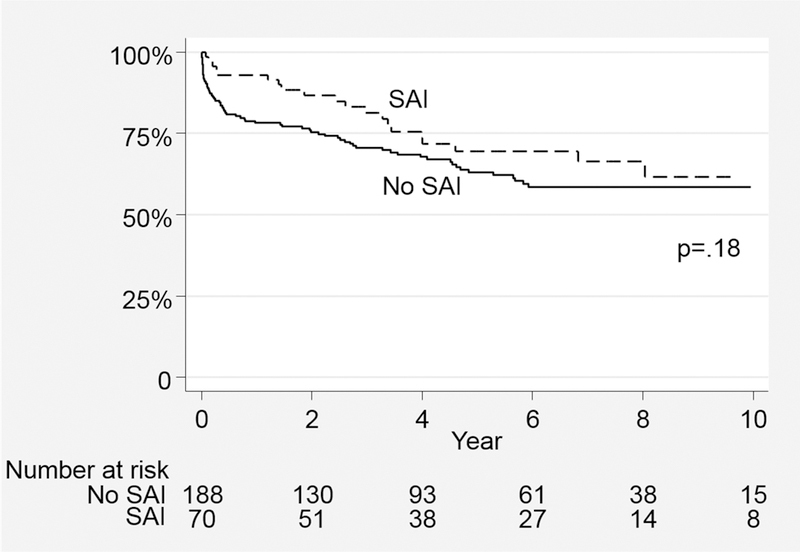
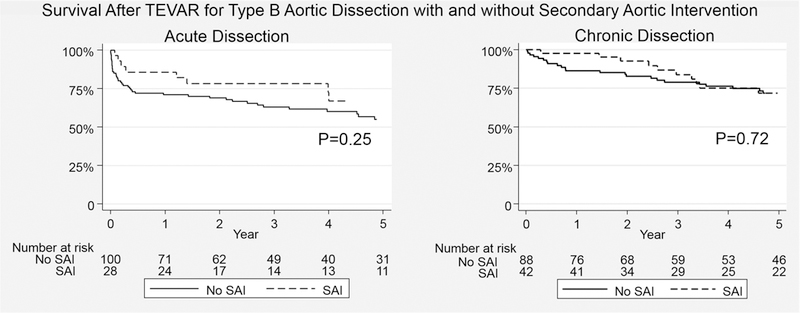
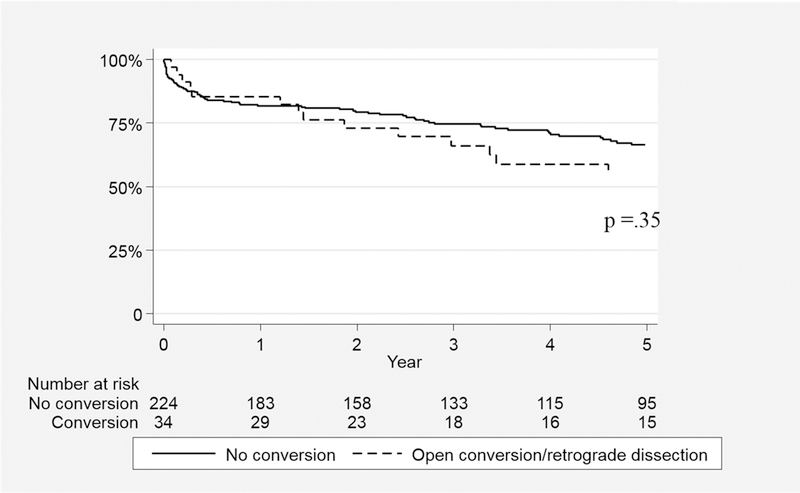
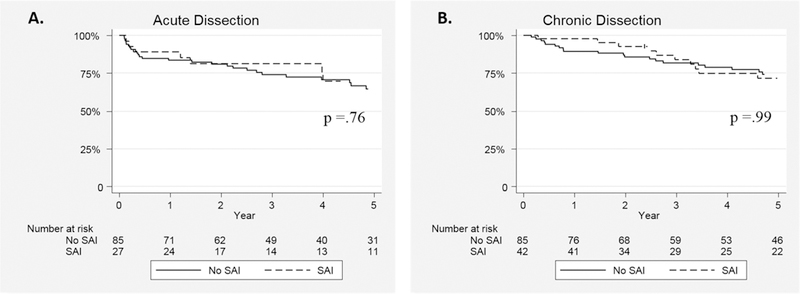
Results: TEVAR for TBAD was performed in 258 patients (acute, 49% [n = 128]; chronic, 51% [n = 130]). Mean follow-up was 17 ± 22 months with an overall SAI rate of 27% (n = 70; acute, 22% [28]; chronic, 32% [42]; odds ratio, 1.7; 95% confidence interval, 0.9-2.9; P = .07]. Median time to SAI was significantly less after acute than after chronic dissection (0.7 [0-12] vs 7 [0-91] months; P < .001); however, freedom from SAI was not different (1-year: acute, 67% ± 4%, vs chronic, 68% ± 5%; 3-year: acute, 65% ± 7%, vs chronic, 52% ± 8%; P = .7). Types of SAI were similar (acute vs chronic: open, 61% vs 55% [P = .6]; major endovascular, 36% vs 38% [P = .8]; minor endovascular, 21% vs 21% [P = 1]). The open conversion rate (either partial or total endograft explantation: acute, 10% [13/128]; chronic, 15% [20/130]; P = .2) and incidence of retrograde dissection (acute, 6% [7/128]; chronic, 4% [5/130]; P = .5) were similar. There was no difference in survival for SAI patients (5-year: acute + SAI, 55% ± 9%, vs acute without SAI, 67% ± 8% [P = .3]; 5-year: chronic + SAI, 72% ± 6%, vs chronic without SAI, 72% ± 7% [P = .7]). Factors associated with SAI included younger age, acute dissection with larger maximal aortic diameter at presentation, Marfan syndrome, and use of arch vessel adjunctive procedures with the index TEVAR. Indication for the index TEVAR (aneurysm, malperfusion, rupture, and pain or hypertension) or remote preoperative history of proximal arch procedure was not predictive of SAI.
Conclusions: SAI after TEVAR for TBAD is common. Acute TBAD has a higher proportion of early SAI; however, chronic TBAD appears to have ongoing risk of remediation after the first postoperative year. SAI types are similar between groups, and the occurrence of aorta-related reintervention does not affect survival. Patients' features and anatomy predict need for SAI. These data should be taken into consideration for selection of patients, device design, and surveillance strategies after TEVAR for TBAD.
Keywords: Aortic dissection; Reinterventions; Secondary interventions; TEVAR; Type B aortic dissection.
Published by Elsevier Inc.
Conflict of interest statement
Figures
Comment in
-
Discussion.J Vasc Surg. 2019 May;69(5):1378. doi: 10.1016/j.jvs.2018.07.085. Epub 2018 Dec 13. J Vasc Surg. 2019. PMID: 30553727 No abstract available.
Similar articles
-
Early Thoracic Endovascular Aortic Repair for Acute Type B Dissection Is Associated with Increased Complications: Results from the Gore Global Registry for Endovascular Aortic Treatment Registry.Ann Vasc Surg. 2025 Sep;118:1-10. doi: 10.1016/j.avsg.2025.03.020. Epub 2025 Apr 13. Ann Vasc Surg. 2025. PMID: 40233894
-
Impact of proximal seal zone length and intramural hematoma on clinical outcomes and aortic remodeling after thoracic endovascular aortic repair for aortic dissections.J Vasc Surg. 2019 Apr;69(4):987-995. doi: 10.1016/j.jvs.2018.06.219. Epub 2018 Oct 24. J Vasc Surg. 2019. PMID: 30528404
-
Efficacy of thoracic endovascular stent repair for chronic type B aortic dissection with aneurysmal degeneration.J Vasc Surg. 2013 Jul;58(1):10-7.e1. doi: 10.1016/j.jvs.2012.12.071. Epub 2013 Apr 3. J Vasc Surg. 2013. PMID: 23561433 Free PMC article.
-
Thoracic endovascular aortic repair for hyperacute, acute, subacute and chronic type B aortic dissection: Meta-analysis of reconstructed time-to-event data.Trends Cardiovasc Med. 2024 Oct;34(7):479-485. doi: 10.1016/j.tcm.2023.12.005. Epub 2023 Dec 23. Trends Cardiovasc Med. 2024. PMID: 38142754
-
Comparisons of open surgical repair, thoracic endovascular aortic repair, and optimal medical therapy for acute and subacute type B aortic dissection: a systematic review and meta-analysis.BMC Cardiovasc Disord. 2025 Feb 7;25(1):86. doi: 10.1186/s12872-025-04478-1. BMC Cardiovasc Disord. 2025. PMID: 39920602 Free PMC article.
Cited by
-
Burden and causes of readmissions following initial discharge after aortic syndromes.J Vasc Surg. 2021 Mar;73(3):836-843.e3. doi: 10.1016/j.jvs.2020.05.080. Epub 2020 Jul 30. J Vasc Surg. 2021. PMID: 32738382 Free PMC article.
-
The characteristics of distal tears affect false lumen thrombosis rate after thoracic endovascular aortic repair for acute type B dissection.Interact Cardiovasc Thorac Surg. 2021 Oct 29;33(5):755-762. doi: 10.1093/icvts/ivab166. Interact Cardiovasc Thorac Surg. 2021. PMID: 34125231 Free PMC article.
-
Physician-modified fenestrated endograft for postdissection thoracoabdominal aortic aneurysm following provisional extension to induce complete attachment and renal artery stenting.J Vasc Surg Cases Innov Tech. 2022 Jun 14;8(3):367-371. doi: 10.1016/j.jvscit.2022.04.015. eCollection 2022 Sep. J Vasc Surg Cases Innov Tech. 2022. PMID: 35898571 Free PMC article.
-
Aortic Root and Distal Arch Management During Type A Aortic Dissection Repair: Expanding Horizons.Braz J Cardiovasc Surg. 2022 Dec 1;37(6):37-6. doi: 10.21470/1678-9741-2021-0178. Braz J Cardiovasc Surg. 2022. PMID: 35657303 Free PMC article. Review.
-
A preliminary ex vivo diffusion tensor imaging study of distinct aortic morphologies.J Anat. 2025 May;246(5):745-756. doi: 10.1111/joa.14223. Epub 2025 Jan 26. J Anat. 2025. PMID: 39865441 Free PMC article.
References
-
- Fattori R, Montgomery D, Lovato L, Kische S, Di Eusanio M, Ince H, et al. Survival after endovascular therapy in patients with type b aortic dissection: A report from the international registry of acute aortic dissection (irad). JACC Cardiovasc Interv 2013;6:876–882 - PubMed
-
- Hanna JM, Andersen ND, Ganapathi AM, McCann RL, Hughes GC. Five-year results for endovascular repair of acute complicated type b aortic dissection. J Vasc Surg 2014;59:96–106 - PubMed
-
- Dake MD, Kato N, Mitchell RS, Semba CP, Razavi MK, Shimono T, et al. Endovascular stent-graft placement for the treatment of acute aortic dissection. N Engl J Med 1999;340:1546–1552 - PubMed
-
- Fattori R, Cao P, De Rango P, Czerny M, Evangelista A, Nienaber C, et al. Interdisciplinary expert consensus document on management of type b aortic dissection. J Am Coll Cardiol 2013;61:1661–1678 - PubMed
-
- Lombardi JV, Cambria RP, Nienaber CA, Chiesa R, Teebken O, Lee A, et al. Prospective multicenter clinical trial (stable) on the endovascular treatment of complicated type b aortic dissection using a composite device design. J Vasc Surg 2012;55:629–640 e622 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
